Dennis M. Dailey
The Sexually Unusual
Guide to Understanding and Helping
1989
Understanding and Helping the Sexually Unusual
Part II: Noncoercive Sexually Unusual Expression
Clinical Treatment of the Cross-Dresser
Women Partners of Transvestites
Clinical Treatment of the Woman Partner
Clinical Treatment of the Couple
Comprehensive Treatment Program
Part III: Coercive Sexually Unusual Expression
Patterns and Characteristics of Offenders
A Model of Sexual Aggression/Addiction
A Treatment Model for Sexual Aggression
Modified Aversive Behavioral Rehearsal
[Copyright]
The Sexually Unusual: Guide to Understanding and Helping has also been published as Journal of Social Work & Human Sexuality, Volume 7, Number 1, 1988.
© 1988 by The Haworth Press, Inc. All rights reserved. No part of this book may be reproduced or utilized in any form or by any means, electronic or mechanical, including photocopying, microfilm and recording, or by any information storage and retrieval system, without permission in writing from the publisher. Printed in the United States of America.
The Haworth Press, Inc., 12 West 32 Street, New York, NY 10001 EUROSPAN/Haworth, 3 Henrietta Street, London WC2E 8LU England
LIBRARY OF CONGRESS
Library of Congress Cataloging-in-Publication Data
The Sexually unusual : guide lo understanding and helping / Dennis M. Dailey, editor, p. cm.
“Has also been published as Journal of social work & human sexuality, volume 7, number 1, 1988”-T.p. verso
Includes bibliographical references and index.
ISBN 0-86656-786-0.
1. Social service and sex. 2. Sex counseling. 3. Sexual deviation. I. Dailey, Dennis M. HV42.5.S52 1988 88–15292
306.7—dc!9 CIP
Dedication
To my partner, Judy, and to my daughters Melisa and Amy, who have helped me to learn how to balance the masculine and feminine in all of us. To my mother, Hazel Andrus Dailey, and to the memory of my father, Floyd William Dailey, who modeled the importance of compassion for others and good humor in life.
Contents
Contributors
Acknowledgments
PART I: BEGINNINGS
Understanding and Helping the Sexually Unusual
Dennis M. Dailey
Historical Perspective
Vern L Bullough
PART II: NONCOERCIVE SEXUALLY UNUSUAL EXPRESSION Fetishism
Fetishism
Thomas O. Sargent
Sadomasochism
Charles Moser
Transvestism
Roger E. Peo
Transsexualism
Sharon B. Satterfield
PART III: COERCIVE SEXUALLY UNUSUAL EXPRESSION Pedophilia
Edward L Rowan
Exhibitionism/Voyeurism
Margretta Dwyer
Obscene Phone Callers
Ord Matek
A Model of Sexual Aggression/Addiction
Steven C. Wolf
A Treatment Model for Sexual Aggression
Timothy A. Smith
Roger W. Wolfe
Afterword
Dennis M. Dailey
Subject Index
About the Editor
Dennis M. Dailey, DSW, is Professor in the School of Social Welfare, The University of Kansas. He is also an Adjunct Clinical Professor, Karl Menninger School of Psychiatry and Mental Health Services and Clinical Consultant, Center for Sexual Health at the Menninger Foundation, Topeka, Kansas. He is certified as a Sex Educator, Sex Therapist, and Supervisor by the American Association of Sex Educators, Counselors and Therapists. Besides his teaching responsibilities, primarily in human sexuality and clinical evaluation, he is active in research, has a limited private practice, and does extensive training and consultation nationally and internationally. Currently, his principle research interest is in variations of male psychological sex-roles in variant life situations. He has authored numerous articles and book chapters relating to human sexuality, sex-role socialization, clinical judgment, and sex therapy. He writes a column regularly for an international journal, The Renal Family, and has special concerns for the many sexually oppressed groups in our society.
Contributors
Vern L. Bullough, PhD, RN, SUNY Distinguished Professor and Dean, Faculty of Natural and Social Sciences, State University College at Buffalo, Buffalo, New York.
Dennis M. Dailey, DSW, Professor, School of Social Welfare, University of Kansas, Lawrence.
Margretta Dwyer, MA, Coordinator, Sex Offender Treatment Program, Program in Human Sexuality, University of Minnesota Medical School, Minneapolis, Minnesota.
Ord Matek, MSW, Associate Professor Emeritus, Jane Addams Graduate School of Social Work, University of Illinois-Chicago, Illinois.
Charles Moser, PhD, Professor, Institute for Advanced Study of Human Sexuality, San Francisco, California.
Roger E. Peo, PhD, Private Practice, Poughkeepsie, New York.
Edward L. Rowan, MD, Private Practice, Concord, New Hampshire.
Thomas O. Sargent, MDiv, MEd, Counselor and Director of Research and Development, The Designed Change Institute, Inc., Hartford; Connecticut.
Sharon B. Satterfield, MD, Director, Program in Human Sexuality, University of Minnesota Medical School, Minneapolis, Minnesota.
Timothy A. Smith, MEd, Co-Director, Northwest Treatment Associates, Seattle, Washington.
Steven C. Wolf, MeD, Co-Director, Northwest Treatment Associates, Seattle, Washington.
Roger W. Wolfe, MA, Co-Director, Northwest Treatment Associates, Seattle, Washington.
Acknowledgments
A special word of thanks to David A. Shore, for his enthusiasm and encouragement about this volume.
The contributors to this volume are deserving of my special gratitude for the able production of each of their articles. Each has written with understanding and compassion, and with a unique expression of self that will make it possible for helpers to see the sexually unusual in some new and different light.
To my partner, Judy, a special thank you for a lifetime of editing my writing and that of others. One day her dogged efforts will hopefully pay off when I write a piece that does not require any sentence reconstruction and embarrassing corrections of my spelling.
To Marian Abegg and Crystal Cunningham I offer my appreciation for the typing and preparation of the manuscript. They worked with true competence and good humor, thank God!
Dennis M. Dailey
Part I: Beginnings
The first two articles in this volume invite the reader to take an understanding and helping perspective on persons who express sexually unusual behaviors, whether coercive or noncoercive. The dominant theme is that services to the sexually unusual must initially adhere to the principle of—FIRST DO NO HARM.
Like all inquiry, it is always enriched by placing it in some historical perspective which broadens our view and forces us to see the evolving and unfolding nature of the human condition. “Historical Perspective” by Vern L. Bullough provides this context, and can sensitize the reader to a humane and caring understanding of the human differences occurring in the sexual dimension of whole persons.
Understanding and Helping the Sexually Unusual{1}
Dennis M. Dailey
One of the more disquieting experiences that can occur in ongoing clinical practice is to encounter client concerns or struggles for which the practitioner lacks preparation or competence in intervention. Many professionals find it difficult to admit publicly, and sometimes even to themselves, that they have little or no idea what to do with respect to a particular client problem. Yet we have all had the experience and have managed it in a number of different ways.
A fair number of clinicians, when faced with this dilemma, essentially “fake it,” hoping the client will not notice, and slowly move the discussion to an area with which the clinician is more comfortable and more competent and prepared to address. This probably accounts for why some clinicians seem to report that all of their clients have essentially the same problem. This is helping dictated by the clinician rather than by the client and the client concern. Others who engage in the “fake it” mode, really do fake it. They leave the client with the sense that they do in fact know something (or even a great deal) about the presenting concern, and essentially experiment or trial-and-error their way through the helping process. This latter mode of operation is the clinical activity which probably strays farthest from the time honored principle in helping—FIRST DO NO HARM. At least in the former strategy the clinician has shifted the work to an area where a problem may exist and for which they have some expertise.
Another strategy for “faking it,” one that is probably less lethal, is where the clinicians recognize that they are “up to their ass in alligators and that they forgot that they went into the swamp to drain it.” They do not necessarily inform the client of the situation, but rather structure a brief time out and begin to look for resources that might give them some notion of how to manage a given client concern. This is clearly a more responsible plan than either of the first two mentioned, even though the client may not know exactly what is happening in the helping process. Critical here is the availability of materials that would give the clinicians some initial leverage on the client problem and allow them to keep one step ahead of the client’s search for growth and change.
Finally, there is the strategy which is most honest, yet difficult for many professionals to allow as a part of the helping process. That is, a straightforward admission on the part of clinicians that they have absolutely no idea or expertise in a given problem area. Persons who operate from this stance tend to do one of two things in an attempt to move the helping process forward. First, is the immediate and intense search for a referral resource to find someone who can help. A second activity, especially if resources are lacking, is to consciously and openly join with the client in a mutual search for information and practice clues that might aid the helping process. Here, both the clinician and the client read much of the same material, or talk to the same consultant, or try the same options in a mutual process.
If there is an area of the human condition that makes the previous introductory comments most salient, it is the area of human sexual function and dysfunction. The vast majority of helping professionals, from all disciplines, have had neither academic nor clinical training in addressing sex-related concerns on the part of the client population. And because the issue is sexuality, it is especially difficult to admit a lack of expertise, since so many of us have a large investment in appearing sexually knowledgeable, skilled, and “cool.” Given cultural dictates, this admission is probably most difficult for males, who are under a lot of pressure to know everything about sex. Professionals do not escape these cultural pressures anymore than do their clients. Many professionals are no more knowledgeable or comfortable with sexuality than are their clients, which in part accounts for why it is so easy for them to join the client in the conspiracy of silence, and results in sex becoming a “hands off” topic in the helping process. It is hard to imagine how much marital therapy is done with little or no attention to the sexual dimension that can so frequently be a part of marital or couple conflict. The client couple may even present sexual dysfunction in a very straightforward manner, yet spend most of their time working on communication or other issues.
Most sex therapists can tell stories for hours about how clients tried to get other helpers to address their sexual concerns, with little or no success. A case in point was a recent consultation with a very skilled marital therapist who was concerned because her work with a couple seemed to be moving so slowly and they seemed so “resistant.” The therapist had correctly assessed that the couple did have difficulty in expressing themselves openly with each other and had been trying to facilitate a more effective pattern of expression. The most dysfunctional communication came about when the couple tried to negotiate their sexual needs, yet no sexual history had been taken and very little discussion of sex occurred in the clinical process. When asked why, the therapist said, “Well, I knew they had some sexual concerns, but I figured if they learned how to communicate better, the sexual thing would get better by itself. Besides, I really don’t know much about helping people with sex problems and it’s not an area I’m all that comfortable talking about.” As it turned out, this couple did have rather serious sexual concerns that needed direct intervention. They experienced very uneven levels of sexual desire. He had been an early ejaculator most of his married life, and the woman was unable to achieve orgasm with any reliability. They were referred for sex therapy, made good progress on their sexual problems, improved their communication significantly, and were returned to the marital therapist who spent a few sessions on some other marital issues before terminating the work. This is not an uncommon occurrence.
There is a small ray of light in the situations described above. In the past decade or so some professional helpers have recognized their deficiencies in training and clinical experience and have sought out opportunities to learn and develop skills in sexuality concerns. Largely, this has been accomplished by seminars and workshops, and has resulted in increased sensitivity and competence on the part of some practicing clinicians. Most of these training ventures have focused on helping clients with fairly typical sexual problems that are experienced by the typical heterosexual, married couple. Included are such concerns as disorders of sexual desire, anorgasmia, erectile and ejaculatory dysfunctions, vaginismus, and dyspareunia. This increased attention is certainly encouraging, but it omits many people who struggle with sexual problems and concerns that would not comfortably fall into this relatively normative group. That is not to say that these fairly typical and normative problems are not painful and serious to those who experience them. It is simply that not all persons fit the standard diagnostic classification found in the DSM III under Psychosexual Dysfunctions (APA, 1980).
One of the first attempts to encourage helping professionals, and in particular social workers, to look at the under or poorly served in terms of human sexuality is to be found in the work of Gochros (1986, 1977, 1972). Gochros identified this group as the sexually oppressed. Included were older people and young people, the physically and mentally handicapped (differently abled), the ill and dying, racial and ethnic minorities, the poor, the homoerotically and bierotically oriented, the single, etc. Sexual oppression arises primarily out of the reproductive bias, which “states that the only acceptable (normal, natural, beautiful, legal, healthy, mature, Christian, desirable, and so on) sexual behavior is that behavior between adults that could lead to a socially approved pregnancy” (Gochros, 1977, p. xx). The list of persons and groups generated is a long one, but a lot of people just do not “fit in” when it comes to society’s definition of sexually normative or those who can conform to the reproductive bias.
There are ... a large number of men and women whose sexual behavior, for one reason or another, could not possibly lead to a socially approved pregnancy. Their needs, therefore, have at best been ignored, and at worst have been prevented from expression. To a greater or lesser degree, we —i.e., significant segments of society —have considered it unlikely, impossible, or undesirable for many of these diverse groups of people to enjoy their sexuality. (Gochros, 1977, p. xxi)
Clearly not all people enjoy the same affirmation for the expression of their sexuality. There is another group of persons, having strong kinship with the sexually oppressed, which has been likewise ignored and who deserve some special attention. They are, what is being called in this volume, The Sexually Unusual.
Who are the sexually unusual? How are they different from the sexually normative? How are they different even from that group identified as sexually oppressed? Like many definitional tasks, differentiating the sexually normative, the sexually oppressed, and the sexually unusual is not easy. The task is initially difficult because the three groups do not represent discrete categories; there is some overlap. For simplicity’s sake, let the following statements suffice.
The sexually normative, or the sexually elite as Gochros (1977) calls them, are persons who can engage in sexual interactions without serious violation of the reproductive bias. That is, persons whose sexual interactions could lead to a socially sanctioned and approved conception and pregnancy. The reproductive bias is a strongly functioning cultural imposition, even in the 1980s, and defines both the sexually elite and the sexually oppressed. The former include the married, heterosexually oriented, young (but not too young), healthy, attractive, economically comfortable, white persons. Anyone possessing these attributes can engage in sexual interactions with relative assurance of receipt of cultural blessing. That is not to say that the sexually elite are without sexual problems and concerns, as was indicated earlier. Sex therapist’s offices are full of such clients.
The sexually oppressed is a large group of persons who cannot easily conform to the reproductive bias and as a group tend to be systematically asexualized. It is not that these persons are in fact nonsexual, but rather that a large segment of society would prefer that they not be sexual, or they are viewed as inappropriately sexual. Most people in our society are, for the most part, reticent to grant the sexuality of the single person, and few people seeing a person in a wheelchair see the sexual dimension of that person.
The sexually unusual are those persons whose choice of sexual expression tends to be viewed in our society as sharply “deviant” or “weird.” They tend to be viewed as either sick or criminal, the latter two categories not always clearly differentiated. For example,
the sexually elite couple, who among other things enjoy oral sex as a part of their sexual interaction, are not generally seen as sick or criminal, and for that matter are not sexually oppressed. A small segment of our society might be bothered by the notion of oral sex, but that is about as far as it goes, even though oral sex cannot be considered essential to the reproductive outcome of sexual expression. Likewise, the couple in their 70s who are very sexually active are not seen as sick or criminal, although society’s repressive attitudes towards older persons being sexual may result in sexual oppression. Sexually active older persons may be scoffed at or labeled “dirty old men” and “little old ladies in white tennis shoes who ought to know better,” and oppressive experiences may result, but that, again, is about as far as it goes. The sexually unusual, on the other hand, are not merely scoffed at or oppressively labeled, but rather are seen as unstable and/or criminal.
Maybe it would help to simply list those persons who are being called sexually unusual in the volume. The list is not exhaustive, but certainly is representative. It includes: pedophilie, fetishist, sadomasochist, obscene phone caller, transvestite, transsexual, exhibitionist, voyeur, and the relatively new group referred to as the sexually addicted. A first observation of this group of sexual expressions yields two fairly clear sub-categories. For example the pedophiliac, obscene phone caller, exhibitionist, and voyeur and some of the persons labeled sexual addicts are clearly sanctioned in legal code and their sexual acts are viewed as criminal due largely to the coercive element in the sexual expression, which makes them clearly intolerable. On the other hand, the fetishist, sadomasochist, transvestite, transsexual, and some persons labeled sexual addicts are not generally viewed as criminal, but rather as just sick and weird. Unfortunately, even this gross differentiation is not usually made, and the sick/weird label for the latter group is clearly unjustified in many cases.
The differentiation process does get sloppy or difficult due to the nondiscreteness of the categories. The sexually normative couple who is into mate swapping, for example, is likely to get the sick/ weird label. Likewise, the sexually oppressed paraplegic male who coerces a sexual interaction will be charged with a violation of criminal code. On the other hand, most couples who express their sexuality through sadomasochistic behavior do so with consent and . as a mutually satisfying and controlled style of sexual expression. Yet, for example, the fetishist who expresses his preference without mutual consent is being coercive and may be in violation of criminal code, although much fetishistic expression is noncoercive.
Another feature of the sexually unusual which differentiates this group from the oppressed and the elite is the male/female proportion of persons involved in the sexual expressions. Without question the larger proportion of persons in the sexually unusual group is male. Most, but not all, pedophiliacs, fetishists, transvestites, exhibitionists (this one is a bit tricky because our society may actually sanction female exhibitionism), and voyeurs are male, whereas sadomasochists, transsexuals, and sexual addicts are somewhat more represented by both males and females, although the larger proportion is still male in these groups. It is not yet clear why this gender imbalance occurs as it does, but a reasonable line of conjecture would have to include the profoundly sexist undercurrent that flows in our society.
Finally, it might be useful to look at how the psychiatric and mental health community looks at sexuality and sexual concerns via the DSM III (APA, 1982). It is interesting to note that both the sexually elite and the sexually unusual are to be found in the DSM III, whereas the sexually oppressed are not recognized as a discrete category. Psychosexual disorders, the major category heading, contains four sub-categories: gender identity disorders, paraphilias, psychosexual dysfunctions, and other psychosexual disorders. The sexually elite are to be found in the category psychosexual dysfunctions, although both the sexually oppressed and the sexually unusual experience sexual dysfunctions. Unfortunately, for both of these groups, the sexual dysfunction is likely to be a secondary diagnosis, with their status as a member of a sexually oppressed group or their sexual unusualness being primary. Most helping professionals who deal at all with sexuality concerns, other than a few specialists and special programs, focus on helping the essentially sexually elite manage the sexual problems they encounter. These include: inhibited sexual desire, inhibited sexual excitement (primarily erectile dysfunction), inhibited female orgasm (anorgasmia), inhibited male orgasm (retarded ejaculation), premature ejaculation, and functional dyspareunia and vaginismus. The sexually unusual are to be found largely in the category of paraphilias, with transsexualism in the gender identity disorder category. A simple reading of the psychosexual dysfunctions compared to the paraphilias will reveal the different stance taken towards these two groups of sexual issues. The treatment interventions for the psychosexual dysfunctions are aimed primarily at the sexually elite. Lots of people in general, and most helping professionals, would not have any difficulty understanding why a married man who experiences erectile failure should receive help with that problem. Offering the same service to a homoerotically oriented male in a primary relationship is viewed with a good deal more skepticism by most people, including many helping professionals. Offering the same service to a male in a sadomasochistic relationship would seem even further out of bounds. It is safe to say that most helping professionals probably know a good deal less about how to be useful to the sexually oppressed, although a recent book by Gochros, Gochros and Fischer (1986) is instructive, and even less is generally known about how to be helpful to the sexually unusual.
To date it would appear as if the sexually oppressed have been viewed as the polar opposite of the sexually elite. Yet, the sexually unusual, for the most part, would be viewed as more non-normative than the sexually oppressed. This discussion would suggest that the sexually unusual represent the polar opposite, both in terms of what we know about the sexual expressions and what is offered in the attempt to be helpful.
One final observation related to the definitional task. There is a good deal of conceptual slippage when it comes to those persons who are being identified as the sexually unusual. Some theorists and clinicians tend to treat all or most of the paraphilias as if they are essentially the same entity, both in terms of etiology and intervention. For example, many of the treatment programs which deal with the sexual addict or the sexually unusual behaviors which fall into violation of criminal code tend not to differentiate causality. As a result, most of the people go through very similar treatment programs.
In other instances, there is some differentiation regarding etiology and some differentiation in terms of intervention strategies. The question really is whether there is but one basic sexual issue or many different sexual issues. Do the pedophiliac, exhibitionist, and voyeur, for example, have some common etiological factor(s) which would suggest a single intervention strategy, or are they each distinct, requiring distinct treatment strategies? And, of course, irrespective of the causal arguments, there is a good deal of disagreement with respect to treatment strategies, most of which have not yet undergone serious study of outcome results and few controlled comparative studies which focus on relative effectiveness. To some extent, the contributors to this volume reflect some of the essential issues raised above.
There is also a good deal of debate regarding whether it is correct or accurate to categorize all of the sexual behaviors now placed in the paraphilia section of the DSM III. For example, do exhibitionistic and sadomasochistic sexual expressions have so much in common that they both require categorization as paraphilias, or are they enough different that separate categorization would be justified? Or even further, should some sexual expressions be removed from the diagnostic nosology all together, in the same way homosexuality has been removed? Should the couple who engages in sadomasochistic sexual interactions as a regular and essential aspect of their mutual and consentual sexual bond be viewed similarly enough to the exhibitionist, who exposes his genitals to children, so as to place them both in the paraphilia category? Many would argue that such a categorization is inaccurate and a residual of our society’s attitudes towards what is defined as “normative” sexual expression. Others would say that both exhibitionists and sadomasochists are “deviant” or “sick” and need intervention directed to change towards more “normative” sexual expression.
This lack of differentiation and confusion around essential definition has probably resulted in some very unhelpful activities on the part of helping professionals. An analogy might be the issue of homoerotic preferences. Although homophobia is still active in the social fabric of our society, many professionals no longer subtly, or not so subtly, try to change the gay or lesbian person “into” a heterosexual. But it is clear that many still harbor such understanding and attitudes, making their intervention efforts far less than helpful. This same issue probably effects such sexual expressions as transvestism, fetishism, or sadomasochism. There is a strong push to move these persons to more “normative” sexual expression, as opposed to addressing the sexual or other concern that might be presented, i.e., helping the sadomasochistic female achieve orgasm as a part of her sadomasochistic sexual life style with her partner, or helping the transvestite and his partner to resolve issues related to his transvestite preference, including working towards a mutually satisfying integration of the sexual behavior.
Many helping professionals will periodically encounter persons who would be considered sexually unusual. The concern of this volume is to provide information that will guide the helping professional in understanding and helping these persons in the best of all possible ways given our knowledge to date. The social work perspective, and for that matter the basic principles underlying much helping, would dictate that the sexually unusual receive the best possible care and concern of the helper. Personal sexual knowledge, personal sexual comfort or preference, and personal sexual competence must not be barriers to providing the help that is needed. Fostering treatment and care for the exhibitionist or pedophiliac, as opposed to years of only incarceration and punishment, is an ethical duty. Helping the fetishist or sadomasochist couple understand and accept their mutual sexual gratification without shame or guilt is equally an ethical obligation. Many sexologists have heard too many “helping” professionals suggest that the pedophiliac be locked up and the key thrown away. And too many have tried to “fix” a sadomasochistic or fetishistic sexual preference, instead of helping to affirm and integrate the expression of such a preference. Other helping professionals just could not understand why one would try to assist a couple to integrate the man’s transvestite preference as opposed to simply suggesting “it can’t be changed; you might just as well get a divorce.” Even others state very openly their unwillingness to work with certain kinds of sexual issues, for all kinds of reasons that are never very clear, just personal.
If the sexually elite who struggle with sexual dysfunctions need our help, if the sexually oppressed need our advocacy and help, then the sexually unusual need the caring attention of the helping professions. This volume is designed as a guide to understanding and helping, and if used as a reference may move helping professionals to operate within the proposition —FIRST DO NO HARM.
References
American Psychiatric Association. (1982). Desk reference to the diagnostic criteria from the Diagnostic and Statistical Manual of Mental Disorders (3rd edition). Washington, DC: American Psychiatric Association.
Gochros, H.L., & Gochros, J.S. (Eds.). (1972). Human sexuality and social work. New York: Association Press.
Gochros, H.L., & Gochros, J.S. (Eds.). (1977). The sexually oppressed. New York: Association Press.
Gochros, H.L., Gochros, J.S., & Fischer, J. (Eds.). (1986). Helping the sexually oppressed. Englewood Cliffs, NJ: Prentice-Hall.
Historical Perspective{2}
Vern L. Bullough
The norms of what constitutes “proper” sexual behavior are culturally defined. Generally in western cultures these norms have been set by the western Christian tradition, even for those peoples and groups in western culture who are not Christian. The norms were only partly biblical. Primarily these came to us through the formtilators of what came to be Christian doctrine. In this sense St. Augustine (d. 430 A.D.) was the most influential. It was he who taught that sex should only be engaged in for the purpose of procreation, and only with the female on her back and the male on top. All nonprocreative sex was sinful (Bullough, 1976).
In traditional western Christian culture then almost all kinds of sexual activity could be labeled as sinful, and what the Church labeled as sinful later came to be called deviant, bizarre, perverted, or unusual. Lest St. Augustine be regarded as out-of-date and passé in today’s world, his concepts remain the course of religious opposition to contraception, and it was his ideas and those of similar Christian formulators which led to legal prohibitions against homosexuality, sodomy, masturbation, and any number of other sexual activities.
Even though the Augustinian position has been more or less traditional in western culture, this did not prevent individuals from engaging in various forms of sinful behavior. Though the Church felt it was important to specify in some detail what was forbidden conduct and to make some sexual activity more sinful than others, in general there came to be a lumping of categories into such groups as the sin against nature or in legal codes the crime against nature (Bullough and Brundage, 1981). Other catch words came to be sodomy, and buggery, but these remained generalized categories and almost any sexual activity not meeting the Augustinian standards could be included in the crime against nature while sodomy not only included anal intercourse but any same-sex activity. Though buggery was usually more narrowly defined as anal intercourse, it too sometimes allowed for a wide latitude in interpretation including bestiality.
In the nineteenth century both the courts and medical practitioners felt a need to be more precise about sexual activities. The result was greater emphasis on sexual activity in forensic medicine, and the beginning of a trend which has tended to label an increasing number of sexual activities as paraphilias. The number of these are dependent upon how descriptive one wants to be. Paraphilia is a term derived from the Greek, para, beyond the usual, and philia, love. More technically a “paraphilia” might be defined as an eroto-sexual condition of being recurrently responsive to, and obsessively dependent on, an unusual, personally or socially unacceptable stimulus, perceptual or in fantasy, in order to have a state of erotic arousal initiated or maintained, and in order to achieve or facilitate orgasm (Money, 1985, p. 147).
The most significant figure in the movement to give greater legal and diagnostic precision was Richard von Krafft-Ebing (1849–1902) who in his Psychopathia Sexualis (1894) expanded far beyond what his predecessor (Casper, 1864) had done. Krafft-Ebing popularized the term “homosexual” and coined such terms as “sadism” and “masochism” as well as several others in order to differentiate one variation in sexual activity from another. Others joined in. Magnus Hirschfeld (1910), for example, invented the term “transvestism,” literally cross dressing, although for a time the Havelock Ellis (1936) term “Eonism” for the same phenomenon was also popular. The term “transsexualism” appeared in 1949 (Cauldwell, 1950). In recent years John Money has served as sort of a twentieth century Krafft-Ebing, distinguishing a number of paraphilias based on what he calls different developmental love maps. He has a propensity for Greek terms rather than Latin or English ones and among his additions are “acrotomophilia” (desire for amputee partner), “mysophilia” (lover of filth), “olfactophilia” (aroused by smells) et al. (Money, 1985, pp. 137–148). Both historically and in current clinical practice, the paraphilias are more likely to be noted in men and boys than women and girls. We are not certain why this is the case. Some have hypothesized that males, because they are more erotically aroused by what they see, unlike women, who are aroused more by what they feel through their skin, means that it is easier to give erroneous signals to males than to females.
Just how many of these variations in sexual behavior are culturally influenced is not always clear. Cross dressing or transvestism is common to both sexes but it appears to be more erotically arousing to males than females. Is this because women are permitted and encouraged to wear many things associated with males while men are more stigmatized if they wear that which is associated with women? Are we more harsh toward boys acting as girls than girls acting as boys because women as adults traditionally have lower status in society than men and, thus, people understand and empathize with females trying to gain status but want to punish males who seem to desire to lose status? Even though the Bible (Deuteronomy 22:5) forbids men to wear that which belongs to women and women that which belongs to men, we know that in the medieval Christian church, a number of women who had lived as men and whose true sex was only uncovered on their deaths were made saints. No man who lived as a woman, however, was ever made a saint, and if such conduct was known or suspected there was punishment (Bullough, 1974).
Some erotic behaviors are clearly associated with current lifestyles and probably never existed in the past. Mysophilia, for example, can probably only be an erotic turn-on when it is possible for people to be clean, which is something that has been possible only in comparatively recent times. It seems hard to imagine that dirt would be a special erotic stimulant to those who saw dirt and grime as ubiquitous, almost impossible to avoid. Would it have been possible for one to be an auoniepiphiliac (lover of diapers) before the existence of modern diapers? Does the paraphilia change when Pampers became the norm? Do we have an auoniepipamperphilia? Because we have a tendency to draw finer and ever more restrictive distinctions, people labeled or stigmatized as belonging to one sexual minority in the past might now be classed as belonging to another.
A good illustration of this is that of a case of a homosexual written up by W. L. Howard (1897). In his self-description to Howard, the patient wrote:
I can define my disposition no better than to say that I seem to be a female in a perfectly formed male body, for, so far as I know, I am a well formed man, capable of performing all of man’s functions sexually. Yet, as far back as I can remember, surely as young as five years, I seemed to have the strongest possible desire to be a girl, and used to wonder if by some peculiar magic I might not be transformed. I played with dolls; girls were my companions; their tastes were my tastes; music, flowers, and millinery interested me and do this day. I have had little sympathy with boys or men. It has always been a topic for thought and speculation, the abnormal development of man. Any such thought or conversations kindles the fire of passion in my brain. My love for a woman is the same that I have for a work of art; for a statue ... (Bullough, 1987)
Though the patient wanted to have sex with other men, thus, technically he was a homosexual, probably today if the patient presented himself to a sex professional, he would be diagnosed as a transsexual. Part of the difficulty is that homosexuality as it originally entered the medical and psychiatric literature (Westphal, 1869) included some of the same characteristics included in the case history cited above. Because of this we have to wonder whether the person diagnosed as a homosexual in 1897 would act differently from a person who identifies himself as a gay male today.
This raises a rather troubling question about the whole historical nature of paraphilias and variations in sexual behavior, namely just how much the cultural definition of what constitutes a specific form of sexual behavior affects that behavior. Did the homosexuals in 1897 accept Howard’s client as one of their own because this is what the person was labeled or did they object and say I am different from that person and if this is what a homosexual is then I am
not a homosexual? How much does accepting an identity of being homosexual today reflect either what is acceptable to the gay culture or what psychiatrists say gays should be like rather than any innate drive?
Two specific areas of sexual behavior, can be used to illustrate just how much the culture of the erotic minority group tends to influence the behavior of those labeled as belonging to that group.
The first example is transvestism. Though Hirschfeld (1910) defined transvestism and described it, the most influential voice for Americans, and perhaps for much of the western world in defining it, has been Virginia Prince. Virginia Prince is a biological male transvestite from Los Angeles who has spent the last twenty years or so of her life living as a woman (I will use the pronoun her to refer to Prince simply because this is how she conceives of herself and how I conceive of her). Prince has been what might be called an entrepreneur of transvestism and in the process she has more or less defined transvestism in terms of her own beliefs. She was able to do this because she was one of the first transvestites to go public, to give talks about transvestism, proclaim herself a transvestite. She published a magazine, Transvestia, a newsletter, the Femme Mirror, and established organized groups of her readers in this country and abroad. Though cross dressing existed prior to Prince’s writing, there was no organized movement. Many transvestites existed on the fringe of the gay movement and the topic was generally absent from the psychiatric, psychological, or medical literature. Prince emphasized that the transvestite was a heterosexual male who used his cross dressing to express the feminine side of his persona.
Eliminated by definition from the category of transvestite were homosexuals, female impersonators, and would-be transsexuals. Each issue of her magazine emphasized her definition and though among her many readers there were those who did not conform, they undoubtedly soon tried to do so. Official chapters of her organization excluded homosexuals and transsexuals. Prince, however, went further. Simply wearing parts of what is considered a woman’s costume was not enough. She emphasized the importance of learning the role of women so thoroughly that ultimately the person could pass as a woman. She recognized that this would be easier for some than for others, but through classes and instructions on How to Be a Woman Though Male (1966), many a transvestite set this as a goal.
As more transvestites left their closet and came together in groups, not all agreed with Prince and rival groups were established which did not quite conform to Prince’s definition. Still, the essential elements in what is regarded as transvestism today are highly influenced by Prince’s definition, and this definition which emphasizes the expression of the feminine other self is quite different from that developed by Hirschfeld or Havelock Ellis.
A similar redefinition has taken place in terms of sadomasochism through the organization of S/M groups in both the gay and straight communities. Until the last decade or so, as Tom Weinberg (1987) has pointed out, sadomasochism was treated in much of the literature as an individual phenomenon, and the interactions between and among people were not examined. Recent research, however, has emphasized that sadomasochism is dependent upon meanings which are culturally shared, learned, and reinforced by participation in the S/M subculture. One recent researcher (Kamel, 1980, 1983) saw the emergence into the S/M culture, at least for a person from the gay community, as a social process, involving a six-stage process. The first step he entitled the disenchantment stage during which an individual becomes disillusioned with the gay world because most of the men he meets are not masculine enough or do not appear to be masculine enough. The result of this conclusion is often depression about being gay. The man then hears about or his curiosity is stimulated by the hyper-masculinity of the leathersex subculture. Gaining courage from this he pulls himself from the closet of depression by his attraction to this new subculture about which he learns the norms and values and is aroused by its erotic possibilities. This is then followed by a drifting phase in which the man searches for partners. Ultimately, he becomes socialized through actual participation, able to establish his own limits on what does and does not fulfill him.
Though these six steps might vary from individual to individual, and sometimes several stages are combined, they emphasize the socialization process inherent in many of the paraphilia of today. One’s identity is defined by the community which is operating in a
particular historical time period and by the various cultures or subcultures in which one operates.
Sometimes the change is only within the various subcultures, as it might be with gay sadomasochism, but other times there is a massive cultural shift. This is perhaps best emphasized by the changes in attitudes toward pornography from the nineteenth century to the present. Technically pornography, literally the writings of prostitutes, is as old as artistic representations and in its written form as old as writing. Greek literature, for example, has a number of accounts dealing with the erotic adventures of prostitutes, and representations of female figures which were at one time classed as pornographic, have been found in vast quantities in pre-literate culture. There are “pornographic” representations on medieval manuscripts and in Renaissance painting. The great age of pornography was the last of the eighteenth century with such classics as Fanny Hill, and there was a further explosion of it in the nineteenth century. The nineteenth century, however, also saw the rise of censorship designed to prevent the circulation of pornography although that did not stop its production. There was postal censorship, prosecution of publishers, and harassment of writers. Contraceptive information was censored and prohibited from distribution because it was labeled pornographic, and even books about sex, such as the works of Krafft-Ebing, were condemned for being pornographic. Whether these views represented only a small minority or reflected the majority view is uncertain, but if it was a minority it was a politically powerful one. Today pornography, in spite of the Meese commission report, has been widely accepted. The best evidence for this change is the rise of the X-rated VCR film and the appearance of more openly sexual scenes on such popular television series as L.A. Law, St. Elsewhere, Moonlighting, and others (Kendricks, 1987). Obviously not all Americans agree on pornography but the vast majority are accepting of it, particularly if it is read or viewed in private.
Though some forms of sexual conduct do not change over the years, there are cultural variations. Sometimes the change is due to the availability of sexual objects. A good example of this is the recorded decline in sexual contacts with farmyard animals, one of the sexual “crimes” which was fairly common in colonial America. For example, on September 8, 1642, a certain Thomas Granger was burned in a pit in Plymouth colony after he confessed that he had engaged in “buggery” with a mare, a cow, two goats, five sheep, two calves, and a turkey (Records, 1855–61, pp. 474–75).
The reason for the decline is quite simply the urbanization that has taken place in modern America which limited access to farm animals, although one has to be cautious in making too vast a generalization. This was brought home to me by a personal experience some twenty years ago when I recounted the above incident to a group of probation officers in a rural area of Los Angeles County. In speaking of the colonial incident I remarked that the appearance of a turkey in this list was somewhat unusual since sex with birds at any time seemed to be rare. My audience, however, who had clients who raised chickens, proceeded to demonstrate how naive I was. One case told by one of the officers which I remember vividly was that of a woman who had a pet chicken. She had an argument with her boyfriend and he, perhaps as a means of getting even with her, went out and more or less raped the chicken. Fortunately, the hen recovered and the couple eventually made up. They again quarreled and the same thing happened but this time the chicken died. She brought charges of bestiality against the man and he was sent to jail. Obviously sex with birds does continue to take place but because of opportunities and availability it is much less likely to do so than in the past.
Even in heterosexual love play what constitutes acceptable sexual contacts varies from time period to time period. Perhaps a good illustration of this is cunnilingus, or oral contacts with the female genitalia. This is rarely mentioned in the sources of the past and was apparently frowned upon although penilingus or oral genital contacts with the male sex organ was frequently mentioned. In today’s society, however, cunnilingus is quite common, so much so that no one today regards it as stigmatized behavior. One reason for the change might well be the improvement in sanitation and personal hygiene which has been a mark of the twentieth century. Another reason might simply be that the culture now permits pleasure for women.
If popular attitudes change so do official attitudes. The best example of this is the change, in the American Psychiatric Association’s Diagnostic and Statistical Manual’s treatment of homosexuality. By a mere change in wording in 1973, thousands, some would say millions of people, were no longer regarded as sick (Beyer, 1981).
What this discourse emphasizes is the importance of not making snap judgments about the sexual behavior which might be observed in either an individual client or a group of clients. What is needed is an understanding of the culture or subculture in which such behavior takes place, and the sequellae of the act. Today’s society is more deeply concerned about unwilling sex partners, i.e., those who do not want to engage in the sexual activity, such as spousal rape, a growing category of criminal activity. American society seems to be willing to tolerate various kinds of sexual activity between or among consenting adults. They are not willing to tolerate sexual activity between adults and children, activity in which one member is an unwilling or hostile partner, and activity which is non-normative, i.e., offensive, should best be done in private. There are still behaviors which are acceptable in some areas and among some groups but not among others. In sum, attitudes toward sexual variations are strongly influenced by the cultural setting and the professional who tries to deal with clients who have engaged in many of the variant forms of sexual activity should make a special effort to understand these cultural variations in dealing with his or her clients.
References
Beyer, R. (1981). Homosexuality and American psychiatry. New York: Basic Books.
Bullough, V. L. (1974). Transvestism in the middle ages. American Journal of Sociology, 79, 138.
Bullough, V. L. (1976). Sexual variance in society and history. Chicago, IL: University of Chicago Press.
Bullough, V. L. (1987). A nineteenth century transsexual. Archives of Sex Behavior, 16, 81–84.
Bullough, V. and Brundage, J. (1982). Sexual practices and the medieval church. Buffalo, NY: Prometheus Books.
Casper, J. L. (1864). A handbook of the practice of medicine. Translated by George William Balfour, 4 vols. London: New Sydenham Society.
Caudwell, D. 0. (1950). Questions and answers on the sex life and sexualproblems of transsexuals. A reprint of an article in Sexology, (1949), 16, 274–280, Girard, KS: Haldeman-Julius Books.
Ellis, H. (1936). Studies in the psychology of sex. 2 vols. Reprint. New York: Random House.
Hirshfeld, M. (1910). Die transvestiten. Berlin: Alfred Pulvermachier.
Howard, W. L. (1897). Psychical hermaphroditism. A few notes on sexual perversion. Alienist and Neurologist, April, 1–8.
Kamel, G. W. L. (1980). Leathersex: Meaningful aspects of gay sadomasochism. Deviant Behavior, 1, 171–191.
Kamel, G. W. L. (1983). The leather career. In T. Weinberg and G. W. L. Kamel, (Eds). S and M: Studies in sadomasochism (pp. 197–203). Buffalo, NY: Prometheus Press.
Kendricks, W. R. (1987). The secret museum: Pornography in American culture. New York: Viking Press.
Krafft-Ebing, R. von (1894). Psychopathia sexualis. Translated from 7th enlarged and revised German edition by Charles G. Chaddock. Philadelphia: F. A. Davis.
Money, J. (1985). The destroying angel. Buffalo, NY: Prometheus Books. Prince, V. (1966). How to be a woman though male. Los Angeles: Chevalier Publication.
Records of the Colony of New Plymouth 1855–1861. Edited by Nathaniel Shurtleff. Boston: William White, Printer of the Commonwealth.
Weinberg, T. (1987). Sadomasochism in the U.S.: A review of recent sociological literature. Journal of Sex Research, 23, (February), 50–69.
Westphal, C. (1869). Die contrare sexualempfundung. Archiv fur Psychiatrische Neurenkrankenheit, 2, 73–108.
Part II: Noncoercive Sexually Unusual Expression
Several of the sexual expressions being defined as sexually unusual are essentially noncoercive in nature. That is not to say that some of these sexual expressions do not occur coercively, as that is clearly not the case. Like any other sexual expression, they can be mutually concentual or coercive, i.e., marital rape. But to lump all sexually unusual behavior into one category seems a blatant error.
The following articles discuss several of these essentially noncoercive sexually unusual behaviors, and do so from a positive and affirming perspective. Both the nature of understanding and helping are thus different from those behaviors that are coercive. Competent helping will require an ability to differentiate sexually unusual behaviors if harm to people is to be avoided.
Fetishism{3}
Thomas O. Sargent
The paraphilias, especially fetishism, offer the student of human behavior an extensive garden of delights. They are as varied and charming as the individuals themselves, and display the multiplicity of interest and preference implied by the “Sauces and Pickles” chapter of The Joy of Sex, (Comfort, 1972, pp. 157–218). A paraphilia is any learned association between sexual arousal and accidental environmental elements producing a “sexual variation” or “unconventional sexual behavior” (Hyde, 1979, pp. 350–352, and Offir, 1982, pp. 252–254). The association results from continued reinforcement by recurrence of the arousal in relation to the stimulating object or situation, or it results from the sexual equivalent of trauma — intense sexual pleasure (Kinsey et al., 1953, p. 644 ff). This is evidently also the source of those sexual responses which are deemed normal. The paraphilias are largely restricted to the male and are rare in females (Katchadourian & Lunde, 1972, p. 286).
Fetishism is a narrower field of paraphilia, in which the source of stimulation or arousal is an inanimate article such as high heeled shoes, or a choker, or material such as fur, leather, or rubber. Fetishism also includes arousal by parts of the body such as the feet or the hair, and ritualistic elements such as used underpants or stolen rubber. These are similar to the rituals of romantic love, and arousal by means of the genitals or breasts, which are considered normal. As a result of the individuality of human development, there are as many “diseases” as there are individuals, and there are no clear lines between form of sexual response and another.
Fetishism and other paraphilias may arise as the result of direct sexual stimulation by the fetish object as when a small boy lies naked on a fur coat, wears rubber lined pants (Britain), or rides “horsey” on aunty’s high buttoned shoes. More commonly, a paraphilia is accidental, as in voyeurism and in the excitement of urine smells on rubber or in the fact that a rubber coat was stolen. The subject builds an association between arousal and the object over time. Kinsey et al. (1953, p. 644 ff), Tollison and Adams (1979, pp. 266–268) and Hyde (1979, p. 351) describe such development. The definition of fetishism at one time included that the fetish object be necessary for arousal (Katchadourian & Lunde, 1972, p. 286), but now includes those who do not need the object for arousal (Gagnon, 1977, pp. 331–332). This confusion probably results from the patient’s fear that a therapist will interfere with the use of the fetish object, resulting in the patient building a case for its necessity. Most rubber fetishists are aroused by their partners without rubber, but prefer the intensity of the arousal which results when their preferred form of rubber is used.
Fetishism is an area in which the therapist can experience enjoyment in human variety without excessive reaction to personal revulsion. Students can be helped to explore sexual variety in this field, thus equipping themselves to reduce the anxiety of their patients through these examples of harmless sexual variation.
Human beings are endlessly inventive. Just as blind people use their blindness to deal with the environment, all behavior patterns including those which are sexually related are used for their effects. The passive-aggressive rubber fetishist is likely to take the rubber coat of someone he wishes to make a victim, while the passive-dependent rubber fetishist will exchange caresses with the soft rubber. The individual with fantasies of males may visualize penises on the soft rubber, while those with fantasies of females may imagine the softness of breasts gently enfolded in velvet rubber sheeting. These extended associations will quickly become part of the fetish behavior, and therapists and theorists will confuse these originally peripheral elements of the individual’s sexual behavior as the source or cause of the fetishism. Such peripheral elements often become strong life systems which will succeed in keeping the fetishism in place in spite of the client’s determination and the therapist’s excellence. As a result, some sexologists tend to define vari-
ous sexual behaviors by the peripheral purposes for which they are used by the individual. Some such psychological constructs are imaginative (Katchadourian & Lunde, 1972, p. 287). They are usually more interesting and psychologically more substantial and significant than those simple psychosocial associations which were the origin of the behavior. However it is viewed, any sexual behavior has special significance for the psychosocial milieu in which it occurs, and that milieu is always particular to each individual (Schimel, 1971, p. 24 ff). Sexual deviations are meaningless when abstracted and applied to other individuals.
No two fetishists are alike. Among rubber fetishists, for example, some like latex, others like rubber, some like the material on cloth backing while others are turned off by the cloth. There are those who like it dry and velvety and those who like it wet, those who are stimulated by the smell of urine and sweat and those who are fastidious, those who like it tight fitting and those who like it loosely caressing, those who enjoy manual stimulation of themselves and those who like to lie on it, those who prefer it with a partner, others who want it alone, those who prefer a female partner, those who prefer male, and those who enjoy both. Some prefer this or that taste, sound, smell, or feel, and may be turned off by other types of rubber. There are those who prefer rubber gloves, those who like baby pants, book bags, bathing caps, balloons, condoms, boots, bloomers, bathing suits, beach bags, those who desire rubber aprons and those who exist for a red rubber coat with a double back, rubber on the outside and smelling and rustling exactly like their fantasy. Each individual has a fetish unlike any other.
Each human being has a sexual hunger and set of associations required for full gratification unlike any other. It is as varied as a freshly made bed, a bath or shower, red roses on the white fence, after wine or before a smoke, after dinner, movies and dancing, or before the movie, after a fight or during violence, with foreplay or without it, with soft music, loud music, or chocolate ice cream. In some instances these elements are just as ritualized and necessary as any fetish. These varieties are confusing and impenetrable for the therapist who needs an explanation in psychological depth before therapy can begin. For others, this is a refreshing view of human
variability to which a confused client can surrender, and then begin therapy by feeling perfectly normal, no matter how illegal or disruptive his particular behavior may be. In many fetishisms the maladaptations can be major, such as the theft of fetish objects or the unacceptable touching of female anatomy in public, but usually the disruptions are restricted to marriage and partnership problems. There is growing unwillingness to regard such behavior as a problem as long as it is kept between consenting adult partners (Hart, 1966).
It is into the midst of such illegal or disruptive, often life threatening situations, that therapists and moralists press the word “normal,” however they define it. By finding some statistical, psychological, or moral authority, some therapists and most clergy and judges hope to control the misbehavior of the client. The client usually hopes for that also. But it fails. As will be described in detail later, the desensitizing experience of knowing and appreciating all sexual expressions as genuine expressions is the first step toward retaining them where they can be rendered harmless, and eliminating them where they must be eliminated. Through the use of such media as the sexual attitude reassessment (SAR) or the extensive descriptions of behavior given in My Secret Garden (Friday, 1973), or The Joy of Sex (Comfort, 1972), the client can first become stable and empowered by realizing that these supposed abnormal responses are normal (McCarthy, 1977, pp. 245–247). When the client is able to surrender to the universality of variety, when the client is able to accept the behavior as a past learned response, he is in a place from which the responses are deemed normal but undesirable. Then client and therapist are ready to begin their work. For most therapists the First Step of Alcoholics Anonymous (AA), surrender or acceptance, is an understandable beginning.
The inconsequential fetishes lend themselves to be used as desensitization for other clients with far more seriously disruptive sexual behavioral responses. I have been blessed with a rubber fetish which has also been a gift to many of my clients.
I am a rubber fetishist and professional therapist, in that order. This combination has given me a special view of unusual sexual practices both through my own personal experience and as a result
of the large number of other individuals whom I have encountered professionally and personally.
For three decades my lighthearted attitude toward my professional work and my fetish has resulted in acquaintances and patients sharing with me things that they have no reason to share with other professionals, and which they often have had reason to conceal. Although my own interest and involvement as a rubber fetishist skews this presentation, I am delighted to take this opportunity to share with you a perspective on my own and some others’ unusual sexual practices, and to present some dimensions which are rarely, if ever, made available in any sort of scientific literature.
I have learned that a fetish is a different thing to each fetishist. My earliest experiences with other rubber fetishists included the pleasant surprise that I have desires similar to others. Also, I discovered three acquaintances are rubber fetishists, a fact I had not known. I met amusing “disapproval” which included such observations as “Why would he ever like that kind of rubber?” It soon becomes obvious that each of us is different, preferring tight or loose, smooth or harsh, cloth supported or unsupported, smelly or odorless. I use this experience in therapy for all sexual response, and agree that “There is more variety in sexual preferences than in eating preferences.”
Ultimately, the question “Why?” becomes absurd amidst such extensive variability. The associations which comprise the fetish can be of importance, but with so much variety it can be a waste of time to search for them. The causes are configurations of associations which may be useful for me to understand in order to desensitize the revulsion that most individuals have to whatever fetish they may be blessed with, but are useless for the diagnostic purposes for which they are often pursued. Perhaps not surprisingly, when pursuit of the originating associations is carried out with this light attitude, more information is gained for the client.
I have four clear vignettes of memory associated with my early delight with rubber which I present either because they stimulate me in the telling or because they may be important to a therapist or client. One is of a woman with long dark hair playing with my penis by stroking it with soft rubber panties and moving her long hair gently and playfully over it. The whole image is intense and all
involving. It is loving, fun, sexually exciting (I have no image of the state of my penis), secure, and safe. For me, rubber most often provides all of these experiences in one simultaneous concert of sensations. A second image is that of a moment of pleasant security when I pull back the bed covers far enough to place my hand gently on the rubber sheet of my bed in order to exchange the upset of a forgotten and unpleasant encounter with an adult for the quiet tranquillity of the soft rubber and its loving associations. A third image is sliding under the cotton sheet to enjoy the rubber after I have been “tucked in” at night, and then engaging in what my mother called “bouncing up and down,” still my favorite form of stimulation with my face and whole body gently moving over the rubber, skillfully massaging my penis between the rubber and my stomach. Orgasm (without ejaculation in my early years) takes place during the play and the play continues beyond orgasm for its tranquillity and delight. The fourth image is of a birthday, probably my second but possibly my third. It is important because it is after the other three in time, and is definitely in a home that we left about the time of my third birthday. The rubber was in the form of solid rubber animals, smooth and rubber smelling but rather hard and of little sexual use. For me, this sharp but unarousing image dates for me and provides perspective on my early sexual history. By the time I was three I was a full blown rubber fetishist. No raincoat, bathing cap, or pair of baby panties was (or is) safe from me.
The origin of my rubber fetish is obviously at the pleasing hands of an adult. This causes many of the several thousand fellow professionals who have heard my story to attempt to make that encounter traumatic. It was not, in any way. Recently one person tried to have me admit that I might have suffered when I discovered what a horrible thing was done to me, but I haven’t discovered that yet. To underscore the peripheral associations with all sexual practices, there is one result which has caused me difficulty throughout my life. Emotionally, I have, ever since, sought the answer to why she stopped. What did I do? This has certain difficult results in my world today, particularly if I am faced with a gentle woman with long dark hair and brown eyes, and then all my associations run and tell me to do anything necessary to regain this ancient love fantasy. Such oblique associations sometimes are important to a client either
as sources of allied life problems or as extensions of sexual pleasure and fantasy.
Information from almost two hundred rubber fetishists suggests that most such associations begin at puberty, although it may be that earlier experiences are not remembered but are stimulated at puberty. Others reported beginning in very early childhood, similar to me. Several began when cotton sheets were taken away from a bed wetter, leaving direct contact only with rubber. A few report continuing to wet just often enough to keep the stimulating substance around them every night. Some report continuing to enjoy bed wetting as part of the complex of associations, and I often thank my guardian angel (with rubber wings) that I love the tranquillity, sexual stimulation and the initiating female, and that I am not stuck with sexual associations like urine which could cause social problems.
Professional behavior in relation to my rubber fetish was supportive, even if inaccurate. As a child I was told, with great kindness by my mother, that “Dr. Brayton says not to worry about bouncing up and down. He says that you will outgrow it by the time you are twelve.” He, my pediatrician, was warm and kind about it, and I appreciate the impact of his support on my life. I had no inkling of being weird, no guilt, in contrast with many of my fellow fetishists at the hands of their professionals. I hoped that I wouldn’t outgrow it, and I didn’t. My only complaint is how often my mother discovered my rubber supply and quietly removed it. I just hid it more carefully and sought more supplies, like the sheet of soft rubber dam my dentist gave me for some cooked up purpose. By age nine, my grandfather’s raincoat came into the house and I made love to it without ever being discovered. I still have a sheet of rubber from it after fifty years. At the same time I discovered that on rainy days my teacher had an incredibly soft rubber cape, so I often behaved adequately badly to be sent for penance to the “cloak room.” Simply stated, my life involved rubber as a central element from my earliest years, and still does as I enter my sixties. Neither my mother nor professionals stimulated any guilt.
I had one encounter with a psychiatrist regarding my fetish. In college I questioned whether I was overlooking something in my continued delight with rubber. So I talked with a psychiatrist after church one day and we moved into privacy for a few moments. He told me that if I felt guilty (discovering that I was unusual seemed like guilt) I could either lay the guilt to rest or the rubber. Keeping both could be emotionally disruptive. I like this model of offering to eliminate guilt in place of eliminating the sexual practice, and have used it ever since as a therapist. For me, of course, I chose to keep the rubber. Immediately after that I acquired a set of Havelock Ellis’ Studies in the Psychology of Sex (1903/1936), which I read with the same effect of desensitization that is so widely used now in sex therapy. I had experimented with “getting rid” of the “habit” in high school and discovered that the more I tried to cut down on making love to my rubber, the more I did it because it was more on my mind, a fact that I would run into later in AA. In all of this I could only find two reasons to wish to end the “habit,” that I used other people’s rubber coats (usually returning them) and that I consumed so much time in the lovemaking. The latter continued to be extensive, usually a half hour or so, gently loving my whole body and penis, on “cloud nine,” delighted and tranquil, about twice each day. This reverse of the usual male hurried masturbatory practice later pleased my female partners, because I can last a long time, thanks to my extended rubber play.
Another encounter with professionals was my sex education class, in the nineteen-thirties. Nothing there stimulated any guilt, so I suspect that not much was imposed about “normal” sexual behavior. It was during the course of this class that my regular orgasms suddenly included ejaculation, so I had an idea of what was happening when a small amount of slightly bloody ejaculate lay on the white rubber panties I was making love to. I suspected that it was the first breaking through of the ejaculate, and the next was less bloody and more ejaculate, the third, on the next day, was without blood. It was at the same time that I discovered that I could add to my excitement by thinking of the girl across the street while loving my rubber. The class helped me integrate my experiences with my knowledge.
Probably the most significant thing about my rubber fetish is its impact on my personality. It has taught me a base of tranquillity to which I can easily return either through loving my rubber, just touching it, or through other similar associations. In a strange way, my love focus is both outwards and toward myself, so I don’t quite fit the narcissistic mold.
As I work as a therapist and trainer I come, more and more, to be thankful for the learning which has come from my rubber fetishism. I understand the power of association in the human mind, and how, the more I wish to turn off a habit or behavior pattern, the more it is present. My relief of tensions through my rubber fetish has given me understanding of how nonsexual situations lead to sexual, often through the interpersonal meanings for the individual or those around him. In some sex offenders the nonsexual associations, similar to my seeking relief from interpersonal stress by enjoying the delights of my rubber, are the triggering mechanisms of the offensive behavior. If the therapist and client focus on the sexual behavior rather than the peripheral associations, the illegal behavior is more likely to persist. For example, if my use of rubber were illegal, my therapist could assist me best by helping me to find another way to relieve or interrupt my interpersonal stress. The dynamic becomes more complex when I learn to increase my interpersonal stress in order to enjoy my rubber more often. In that common situation, the client and therapist must also address the dynamic between sexual behavior and the peripheral associations.
My rubber fetish has increased my understanding and my flexibility about the meaning of any given sexual response in the lives of my friends and my patients. My delight in rubber is a gift I share with my friends and occasionally with patients. My own ease with rubber is well known among my colleagues. They tease me. They ask questions for their patients. Acceptance needs to go on to unqualified delight. That’s what I enjoy, and that is often what I succeed in communicating to others.
Occasionally I will share a bit of my fetishism with one of my patients. It is socially benign enough to make this possible without risk to me. For example, after allowing a new patient to stumble over presenting his transvestism (“Umm, sometimes, umm, uh, I, uh, putonaskirt”), I smiled and suggested that anyone who wore a cloth skirt instead of rubber was weird. This so disrupted his beliefs about sexuality and his guilt about his transvestism that he left his first session with a delightful self-satisfaction in his transvestism.
Once that was resolved, we could go on with the difficulties of incorporating transvestism into life.
Therapists ask me how to socialize the sexually unusual. I respond that I usually lie a lot in our repressive society. Some patients genuinely wish to make an easier adjustment than deceit, but we do not encourage people to be open when they can be damaged and suggest they discriminate carefully. Sometimes we help them deceive their wives, occasionally with the agreement of the spouse, but more often we help them educate their partners to include the behavior within the relationship.
My own experience with the use of rubber with my partners has been all the way from direct objection to their own separate delight in the soft material. The experience of many rubber fetishists has been similar. Some never learn that an early learned response can never be matched by a present development of sexual association with a fetish. The lifelong involvement with the fetish and the development of extensive associations is specific to the individual and can never be matched by another fetishist or a partner. We human beings are just too individual in our psychological development. However, it is this individuality, this multiplicity of sexual expression, which can be used by the therapist to help the fetishist and partner to more easily accept the unusual.
It is this open attitude both around the office and in myself that has permitted the sharing of many otherwise secrets by clients and colleagues. Clients and friends share with me things they have never shared with others. It is accepted by my closest colleagues and clients that there is no such thing as “unusual” —or rather “usual.” Each of us is a complex of associated behaviors and meanings, some with sexual arousal and some with sexual turn off. No one individual is like another.
In my own presentations of my rubber fetish I do not fail to enjoy some good laughs at myself. This is because I take myself seriously, seriously enough to laugh at things that are absurd. For example, the number of times that I have received disapproving looks from women wearing rubber raincoats who thought I was looking at them, and from men who mistook my absorbed gaze as sexual attraction to them. I go nuts over rubber coats, and will take the time to follow or cross a street just to prolong the delight of sound or vision. Then I will hurry to a place where I can love my rubber while fantasizing about the one I saw. Or I will lay one on top of another, and be very promiscuous by loving the red while fantasizing about the blue, and maybe go to get the blue and become distracted by the black. It’s a delight. One day in a store I watched for a long time as a lady tried on a yellow poncho. She stood and posed in front of a mirror, smoothing the soft rubber over her breasts. I was standing at the rack, touching the same soft rubber. She came over, returning it with a warm smile. Dark hair and brown eyes — the coat was still warm as I scooped it up and bought it. It is still a favorite fantasy. Or the small department store which always had a supply of various kinds of rubber coats (if I don’t have a particular style or color, I must). After years of buying there I was looking for a particular coat in my size. The salesman took me to a private loft upstairs where there were hundreds of rubber coats. I do not know if someone there shared my fetish, but it was my idea of heaven. I took lots of time, so the salesman asked if it was all right if he left me alone. All right? There was a long flight of stairs up to the loft, and I could hear clearly, so I went around my heaven with a delightful erection, and sampled the softness of the rubber against my penis. Every coat in the collection. Then I took a few and laid them on a flat surface and made love to them. It was incredible. I repeated the whole scenario three or four times, but I was a good customer, so there was never any trouble. The last time, just before the store was sold and torn down, I decided on a rack of police raincoats. I arranged them in a line, evenly spaced, and when I came I made sure that I hit all of them, just a little each. So the police in that town have a little of me on their raincoats. So do all those people who are wearing coats that I returned in exchange for another color or size or style. It’s all silly, and fun.
A few friends have even loaned me their rubber coats or rubber gloves, knowing how I was going to use them. One day I was with a friend and someone in her living room started talking about sex. It soon turned to my rubber, and another noticed that I was wearing a rubber shirt. Right away I turned to my hostess and said, “Betty, you know that soft, amber douche bag in the bathroom? It’s no longer a virgin!” These and other stories encourage stories from my friends and patients, but they also support ease with their “peculiarity.” After the wife of a transvestite heard me tell some of my foolish escapades, she went out with him in drag one night to pick up a fast food order. She left him in the parking lot directly under a light for all to see. He went nuts with glee, fear and embarrassment, and suffered only one sexual approach by a male. This helped their ease with his transvestism.
Given the nature of fetishism, it is likely that education, not treatment, is preferable for most purposes. Even when there is extensive disruption of the relationship much more can be accomplished by having each party become clear about what they are and are not dealing with. In the absence of effective sex education courses, especially those which include the all-important SAR, the reading of books similar to The Joy of Sex (Comfort, 1972) will be effective desensitizers. My presentations of my stories and those of others to groups or individuals as appropriate serve the purpose of desensitization. Laughter, particularly at the self, dislodges the judgments and fears that are associated with most sexual behaviors because it provides a new perspective. Such changes in perspective, in how the individual frames the situation, surround all our sexuality work, especially in the earlier sessions. The fetishes offer the therapist the opportunity to dislodge the seriousness which entrenches a distressed perspective, and discover the effectiveness of these approaches even to serious sexual difficulty and offenses. It is also effective. At best, a six foot man looks ridiculous in ten inch heels and knows it. If the therapist can’t laugh, the message is clear to the client that it is as weird as he thought. It only remains for the skillful therapist to help the client understand that he or she is laughing with the client, not at him, and there I have the advantage over you as a result of my fetish. You are invited to use my stories if they will help your work.
We carefully weave at least these four thoughts into early sessions with our clients, always all four developed simultaneously with whatever emphasis seems most effective for each client:
(A) Develop a sense of ease around sexual variety (Schwartz and Masters, 1983, pp. 13, 16; McCarthy, 1977, pp. 243, 244). Encourage education and extended information both in and out of sessions. Encourage the reading of materials such as The Joy of Sex (Comfort, 1972), and suggest attendance at a SAR. Develop a sense of the wide array of sexual variety, somewhat avoiding the presenting problems at first because of their associated meanings and distress. Develop an atmosphere of ease and stimulate laughter (Sargent, 1984, pp. 50, 101). Use this approach regardless of the harmful aspects of the presenting problem, and if this does not make sense to you, visit several AA meetings until it does make sense.
(B) Explore with the client the roles of rigid past learned responses for such things as walking and responding sexually (Sargent, 1984, p. 16 ff). Again, begin the sexual aspects of this strategy in areas away from the presenting problem. Encourage the client to continue to explore and experiment with past learned responses until his or her role in human behavior is learned. Clients quickly discover that past learned behavior patterns quickly take over to control behavior especially powerfully during periods of stress. Emphasize that stress comes in two packages, eustress and distress (Selye, 1976, p. 15). Both forms of stress can mobilize and so strongly entrench a behavior pattern that no other options are available while it runs to its end. This automatic behavior is totally different from aware and intentional behavior, a fact which we use to greatly reduce the client’s experience of guilt. These automatic and unaware responses can gradually be made aware. During periods of ease, automatic responses can be disabled. Powerful inroads against their strength can be made by acceptance of (D) below (Sargent, 1984, pp. 125–126).
-
Cultivate a solid sense of self (Sargent, 1984, pp. 14, 86; Schwartz and Masters, 1983, pp. 4–8). This will become the firm ground from which all work will be done. The client and others are encouraged to explore and identify the self which actually created the behavior patterns which control automatic response today. Specific qualities are celebrated, reinforced, and associated with one another until it all becomes a new learned response. Over time it becomes self-appreciation, self-knowledge and solid self-confidence. Increased clarity about the difference between behavior patterns and the self makes it easier to accept the undesirable things affected by the past learned responses. Increased self-knowledge will discriminate between the self and its qualities and the undesirable qualities which may be contained in some behavior patterns.
The self is author only of present and aware actions, so life begins again each moment. Past responses are past learnings and need not take away from who the self is today even when they run. An effective strategy is the celebration of differences, starting in nonsexual areas, then including the sexual. This helps to identify facets of self that are otherwise unknown. Gradually, the client builds the base from which the work will be done.
-
The universal experience with behavior patterns includes the fact that the harder the pattern is pushed against the more powerfully it will run (Schwartz and Masters, 1983, pp. 8–13). For the alcoholic, the more he determines to not drink the more he will drink. For the fetishist, the more he wants to not use the fetish the more it is on his mind and the more likely he is to use it, as I discovered in my own life. Alcoholics Anonymous discovered surrender or acceptance. Once that occurs, within the ease of acceptance the pattern is less likely to run because of the reduced stress, and the self has more opportunity to develop and put in place other options.
With these tools, more fully described in The Behavioral and Medical Effects of Stress (Sargent, 1984), the client is empowered to select and make changes in his life that suit him. They also provide a multiplicity of options which can be adapted to other sexual problems including dysfunctions. It was this attitude that permitted one colleague to think to offer a premature ejaculator, who had failed in his previous therapy, an inventive approach. He suggested that the individual go ahead and ejaculate immediately as long as he remembered that males are capable of multiple ejaculations while maintaining erection. The client was successful and therapy was terminated. Long therapy had failed for him. Inventive celebration succeeded. Multiple ejaculations are impossible according to some physiologists who know the plumbing, but there are many males who have evidence to the contrary, including me on my rubber. Multiple orgasms are, of course, well known in both males and females.
I will have accomplished much if a few therapists begin to use such ease and delight in their treatment of sexual problems, especially fetishism. I expect that many who use this approach will begin to apply it to other forms of sexual deviation and dysfunction with success. The ease, self-appreciation and acceptance which results is an invaluable ally in the process of any kind of therapy. In the example of erectile failure it is the physiology of emotions which are the cause. Through the skillful foolishness advocated here, and through self-accepting ease, these physiological phenomena can be made to disappear and heal themselves. Kraines (1948) notes that when a patient with erectile failure is advised to not have intercourse for a time, he may soon experience an erection and fulfilling sexual response. We understand this as the result of reduced tension. Likewise, it is in such an atmosphere that the glans squeeze for premature ejaculation or the positions for retaining a flaccid penis in the vagina are most likely to be learned, practiced, and then reported on in the next session with continued amusement, openness to learning, and willingness to explore.
Resources for fetishists are limited. There have been magazines and clubs over the years, such as the Macintosh Society in London and “Latent Image,” which is still available in pornographic bookstores. Some have been supportive of variety and delight, but most have been extreme and exploit the fetishist. Many personal ads have been dangerous and personal contacts have resulted in unwanted phone calls. Such contact can be useful, as it was for me. The pitfalls can be managed by those who are adequately forewarned.
Most porno bookstores carry “Latent Image.” I have not seen “Rubber Life” for years. There are erotic books on fetishism. They still contain parental moralizing by credentialed professionals who disapprove of the behavior which has just been described in vivid detail. This is in order to meet the requirements of the law of past years. These can all be fun, but again, the fetishist must be prepared. There are several sources of rubber and latex clothing, both off the rack and made to order. They are mostly expensive and fun. Of course, for myself and for many other types of fetishists, our source of erotica can be as nearby as the local Salvation Army thrift store.
Readers are welcome to contact me at Designed Change Institute, 3 Columbia Street, Hartford, Connecticut 06106 (Telephone [203] 247–1912) for the most up-to-date information about what is available, or for further clarification about the fetishes. I am also willing to spend a bit of time talking with one of your clients if it would help. Most of all, I hope that you will take foolishness seriously and use it effectively.
References
Comfort, A. (1977). The joy of sex. New York: Crown.
Ellis, H. (1936). Studies in the psychology of sex. Scranton, PA: Harper and Brothers. (Original work published 1903).
Friday, N. (1973). My secret garden. New York: Simon and Schuster.
Gagnon, J. H. (1977). Human sexualities. Glenview, IL: Scott Foresman.
Hart, H. L. A. (1966). Law, liberty and morality. New York: Vintage.
Hyde, J. S. (1979). Understanding human sexualities. New York: McGraw-Hill.
Katchadourian, H. A. and Lunde, D. T. (1972). Fundamentals of human sexuality. New York: Holt, Rinehart and Winston.
Kinsey, A. C. et al. (1953). Sexual behavior in the human female. New York: Saunders.
Kraines, S. H. (1948). The therapy of the neuroses and psychoses. Philadelphia: Lea and Febiger.
McCarthy, B. W. (1977). Strategies and techniques for the reduction of sexual activity. Journal of Sex and Marital Therapy. Vol. 3, No. 4.
Offir, C. W. (1982). Human sexuality. San Diego: Harcourt, Brace, Jovanovich.
Sargent, T. O. (1984). The behavioral and medical effects of stress. Hartford: Designed Charge Institute Publications.
Schimel, J. L. (March 1971). Some practical considerations in treating male sexual inadequacy. Medical Aspects of Human Sexuality, pp. 24–31.
Schwartz, M. F. and Masters, W. H. (1983). Conceptual factors in the treatment of paraphilias: A preliminary report. Journal of Sex and Marital Therapy. Vol. 9, No. 1.
Selye, H. (1976). Stress in health and disease. Boston: Butterworths.
Tollison, C. D. and Adams, H. E. (1979). Sexual disorders: Treatment, theory, research. New York: Gardener Press.
Sadomasochism{4}
Charles Moser
The relation of love to pain is one of the most difficult problems, and yet one of the most fundamental, in the whole range of sexual psychology. Why is it that love inflicts, and seeks to inflict, pain? Why is it that love suffers pain, and even seeks to suffer it? ... [I]f we succeed in answering it we shall come very near one of the great mysteries of love. At the same time we shall have made clear the normal basis on which rest the extreme aberrations of love. (Ellis, 1903/1936, p. 66)
Thus, Havelock Ellis started his discussion of the phenomenon now called sadomasochism (S/M). It is no less intriguing today and, unfortunately, not much more is now known than was known then.
The social stigma attached to S/M is so great that few clients will admit to these interests, for fear of what the psychotherapist or physician will think. As will be seen later, the number of practitioners is so great that it is obvious that all clinicians have contact with S/M practitioners. The lack of understanding of the nature of the S/M subculture and practitioner leads the clinician to make assumptions and errors which may alienate the S/M practitioner-client. The present article seeks to describe the S/M practitioner and the common types of presenting problems encountered by a psychotherapist.
Definition of the Phenomenon
There is no accepted definition of what constitutes S/M behavior and the spectrum of sexual interests of those individuals who adopt an S/M identity is quite broad. Colloquially, we can define S/M as an erotic interest in giving and/or receiving painful (either physically or psychologically) stimulation. It should be noted that the perception of pain is in the judgment of the observer; the recipient may or may not report the experience as painful. From the perspective of the clinician, the colloquial definition is the starting point, though it is clearly inadequate and simplistic. Moser (1979) and Weinberg, Williams, and Moser (1984) discuss the problems with creating an acceptable definition at length.
For the purpose of the present article, an S/M practitioner is an individual who actually takes part in the behavior and self-defines as being involved in S/M or a similar term.[1] Additionally, for the purposes of the present article, S/M practitioners engage only in consentual acts among adults. While members of any group can engage in nonconsentual acts, it has been unfairly and incorrectly assumed that S/M practitioners must somehow be forced or coerced, or force or coerce their partners, into engaging in these activities.
Etiology
S/M has been ignored by most theorists attempting to explain the etiology of sexual behavior. Most of the theory extant is extrapolation of concepts relating to other sexual variances, often developed without the benefit of contact with actual S/M practitioners.
Several theorists have made statements about the etiology of S/M, again without any validation that these theories have any basis even to a clinical sample. An incomplete listing follows: Krafft-Ebing (1886/1965) suggests that S/M is congenital. Freud explains S/M as a transmutation of the death instinct or simply aggression attached to sex (Levitt, 1971). Stekel (1929/1953) suggested that S/M was a form of psychosexual infantilism, while Reik (1941/ 1976) suggested that the masochist is afraid of orgasm or something associated with orgasm. Homey (cited in Levitt, 1971) explains
sadism as a neurotic need for superiority and masochism as an attempt to find safety and satisfaction through dependency, while Deutch (cited in Ford & Beach, 1951) believes that masochism is normal for women. Thorpe and Katz (1948) suggest sadism stems from early condemnation and shaming, and dissipates castration fears. Additionally, they suggest masochism is caused by a desire for superiority. Maslow (1942/1963) suggests that S/M interests develop out of feelings of insecurity. McCary (1967/1973) suggests that S/M interests are a response to feeling disgust for anything sexual or fears of castration. It should be noted that none of these theories has been adequately tested nor has any been shown to apply more to an S/M sample than a non-S/M sample.
There is a considerable amount of psychoanalytic literature on the etiology of sadomasochism (Panken, 1973; Schad-Somers, 1982), and some literature from the behavioral perspective (Annon, 1974/1975). Despite the preponderance of these hypotheses, there is no accepted understanding of what causes an S/M sexual orientation, or for that matter any other sexual orientation, to develop.
As S/M behavior is seen transhistorically (Ellis, 1936) and cross-culturally (Ford & Beach, 1951), we can assume it is part of the repertoire of innate human sexual behaviors. Behavior which appears to be analogous to S/M is also common among mammals. For example, Kinsey, Pomeroy, Martin, and Gebhard (1953) name 24 different mammalian species which bite during coitus. Additionally, Gebhard (1976) remarks “From a phylogenetic viewpoint it is no surprise to find sadomasochism in human beings” (p. 163).
History
Prior to Krafft-Ebing (1886/1965), S/M was neither a sickness nor a sin (Bullough & Bullough, 1977). It seems that behaviors that we might consider to be S/M were commonly found in ancient marriage manuals (Kokkoka, 1150/1965; Nefzawi, 1400/1964; Vatsysayana, 450/1964). It was only in the late fifteenth century that the first unambiguous case report of S/M was reported, and then as a medical curiosity rather than a problem (cited by Ellis, 1936). Other case reports written in a similar vein followed, but S/M was still seen as a curiosity rather than pathology. While S/M behavior prob-
ably existed before the 15th century, historical accounts do not include enough information to ascertain whether the behavior was done consentually and/or for erotic purposes in order to make an unambiguous categorization.
S/M Practitioners
There have been several recent studies of S/M samples, in an attempt to describe the individuals who engage in the behavior (see Breslow, Evans, & Langley, 1985, 1986; Moser & Levitt, in press; Spengler, 1977). These studies have for the most part not found any significant differences between S/M and non-S/M samples. The S/M samples have tended to be better educated and more affluent, but this skew is probably due to who is likely to participate in this type of research project. It is expected that S/M practitioners span all socioeconomic classes and groups. None of the studies was random, so it is not known if all sexual orientations are equally represented. Nevertheless, heterosexual men and women, bisexual men and women, and homosexual men and lesbians are represented in these studies.
There is great diversity on the estimates of the number of S/M practitioners in the general population. At least part of this variance is due to the different ways S/M or similar concepts are presented or defined in these general studies of the sexual behavior. The estimates range from about 50%, those who report at least some erotic response to being bitten (Kinsey et al., 1953), to approximately 5%, those who report obtaining sexual pleasure from inflicting or receiving pain (Hunt, 1974). It is the present author’s best guess that approximately 10% of the adult population are S/M practitioners. This number is similar to estimates of the number of homosexuals in the adult population, but obviously the visibility of these groups is quite different.
There is some question of whether as many women as men are S/M practitioners. This relates to an important theoretical question: Is S/M similar to homosexuality where there are a significant number of men and women involved in the behavior or to fetishism where few or no women are involved in the behavior? The latest
data suggest that a significant number of women are involved in the behavior (Breslow et al., 1985; Moser et al., in press).
S/M practitioners tend to at least try many different sexual behaviors and are not exclusive in their S/M interest (Moser et al., in press). Most report that they do not need to engage in S/M behavior or fantasy to reach orgasm (Moser et al., in press; Spengler, 1977). Though Breslow et al. (1986) asked the question differently and found that for approximately 70% of their sample, orgasm was easier to achieve if S/M was involved.
It is important to note by its absence any indication that S/M practitioners have any common psychopathology or symptoms. While the studies of this population are still sketchy, no consistent picture of S/M practitioners has emerged in the clinical literature. There have been some limited attempts to use psychological testing to see if an S/M sample differs from a control sample. None of these studies shows any significant difference between the S/M group and the control group (Gosselin & Wilson, 1980; Miale, 1986; Moser, 1979).
S/M practitioners report an interest in assuming both the dominant and submissive roles, with relatively few individuals indicating exclusively dominant or submissive interests (Breslow et al., 1985, 1986; Moser et al., in press; Spengler, 1977). There is some indication that more people prefer the submissive role to the dominant role, though they engage in both behaviors, but this is not substantiated at this time.
While there is some disagreement, there is little doubt that at least some S/M practitioners are able to sustain long term relationships. The role of S/M in these relationships varies in a number of ways. Some couples only engage in S/M during some sexual interactions, some always have at least an element of S/M in all sexual interactions, some employ S/M role-plays throughout the relationship but not at all times, and some attempt to live out the S/M roles at all times. Some individuals see S/M as part of foreplay (a sex-style), others see it as part of a lifestyle, while still others fluctuate between these two states (Breslow et al., 1985, 1986).
The roles employed are quite varied. The roles of “master/ slave,” “dominant/submissive,” “guardian/child,” “emplover/ servant,” “owncr/owned,” etc. are distinct and imply different ic-
lationship characteristics and help shape the acceptable acts that take place.
There is evidence that the respondents to the various studies did not believe that their S/M interests were a psychological problem and that they did not wish to change their S/M orientation (Breslow et al., 1986; Moser et al., in press).
While the S/M participants report some concern that their S/M activities will escalate to a dangerous level (Moser et al., in press), this concern seems to be misplaced. Lee (1979) found no incidences of this and no incidences were found after a search of the medical and psychiatric literature.[2]
S/M Behaviors
S/M behaviors can be generally divided into two types, physical and psychological. Usually, S/M practitioners enjoy some combination of these two types, but some individuals are quite specific about which behaviors they enjoy and which they do not. These preferences are not only within groups like physical, but may be as specific as being beaten with a blue whip 2’ 3” long by a blonde woman who speaks soothingly. It should be noted that participation in any of the following behaviors does not mean that an individual is involved in S/M. The following behaviors include behaviors common to some S/M practitioners, but not every S/M practitioner enjoys any or all of these behaviors.
Physical behaviors: The physical behaviors may be further subdivided into the following categories: bondage, physical discipline, intense stimulation, sensory deprivation, and body alteration. These categories are not meant to be mutually exclusive.
Bondage or restraint ranges from being held down or tied in such a manner that the person could escape if he or she tried, to behaviors involving elaborate restraints that leave a person completely immobilized. This category also includes the partial immobilization through the use of handcuffs, leashes, constricting clothes (e.g., corsets), etc.
Physical discipline ranges from slapping to whipping to caning. These behaviors can be of low intensity such that no marks are left, of moderate intensity such that only a redness that will disappear in
a few hours or days is left, or of high intensity so that extensive bruising, welts, or other lesions are left for several days or even weeks. Often, the recipient of these blows does not recognize what level of tissue damage has been inflicted nor does the intensity of the pain experienced necessarily relate to the tissue damage inflicted.
Intense stimulation activities include scratching, biting, the use of ice on skin, hot wax on skin, etc. These are activities that produce strong sensations with little or no tissue damage. The range of these behaviors usually involves duration or manner. Scratching someone’s back a few times can be quite pleasing, but scratching someone’s back for an hour can be quite painful. Also included in this category are any behaviors or devices that increase sensation. For example, a spanking on wet skin is more intense than on dry skin; dropping hot wax from several feet above someone is a very different sensation from dropping it from a few inches above them.[3]
Sensory deprivation can also heighten sensations as well as intensify feelings of vulnerability. For example, a blindfold deprives the wearer of knowing when or where the next blow is to be struck. Not being braced for the blow may increase the sensations as well as focusing the recipient on the sensation without any other distractions. Other examples of sensory deprivation devices include hoods, ear plugs, gags, etc.
Body alteration activities involve tattooing, piercing, branding, bums, etc. While many of these activities are meant to be permanent, they often are not. These behaviors may be seen as proof of S/M commitment, beautifying, or as sensory enhancements.
It should be noted that the activities that cause more physical damage have the lowest frequency (Moser et al., in press). S/M practitioners want to engage in the behavior. If the behavior disabled the recipient, then that person would not be available for S/M interactions in the future. In addition, the dominant partner would gain a reputation for “going too far” and other submissive partners would be hesitant to become involved with that dominant. The result is that most S/M organizations stress and teach safety, and serious injury is rare.
Psychological feelings: Psychological pain is induced by feelings of humiliation, degradation, uncertainty, apprehension, powerlessness, anxiety, and fear. These feelings are often triggered by specific acts for each individual. In the S/M subculture the most common psychological aspect of the interaction is humiliation, but there is no behavior that is universally humiliating to everyone. It is important to note that some people would find submission very humiliating and not desire it, while obviously some people seek out this feeling. Given that not everyone has the same likes and dislikes, it should not be surprising that S/M participants view these feelings differently.
These psychological feelings are generated by both verbal statements and actions taken. For example, verbally berating the submissive (e.g., “You are a poor excuse for a slave”), requiring the submissive to do menial or embarrassing acts (e.g., clean the toilet or kissing the dominant’s feet), being left alone in a vulnerable position (e.g., being left alone without money, keys, or identification), etc.
Both physical and psychological behaviors are devised to emphasize the transfer of power from the submissive to the dominant partner. S/M practitioners often report it is this consentual exchange of power that is erotic to them and the pain is just a method of achieving this power exchange.
Types of Clinical Problems
S/M practitioners, like members of any other sexual orientation, can have psychiatric problems. These problems may or may not have any connection to the individual’s sexual interests. The determination of whether S/M interests are causing, exacerbating, or irrelevant to the problem is difficult, and requires considerable knowledge of the S/M community and the spectrum of S/M practices. Given that there are few experts on sadomasochism, a non-judgmental approach and a desire to learn more about S/M is essential to anyone dealing with S/M practitioners. Recognition that S/M is not a comfortable subject for the clinician is adequate reason for referral.
The following are types of problems that the author has seen in approximate order of the most frequent to least frequent complaint. Obviously, the reputation of the author would tend to cause some prospective clients either to seek out or avoid the author. Therefore, the ordering should not be construed as a reflection of the actual incidence of the problem among S/M-identified individuals.
-
Am I normal? By far the most common and easiest problem with which to work, is this one. Many people beginning to explore their S/M desires are concerned that S/M is a pathological condition that leads people to commit heinous crimes and will be detrimental to the quality of their life. It is common for S/M practitioners to believe that their interest in S/M will escalate to a point where dangerous activities are commonplace, and major injury is just a matter of time. In fact, this is false; few injuries result from S/M interactions (Lee, 1979).[4] Reassurance, education, and referral to a support group often solves this problem in as little as one session and rarely more than six sessions.
Untreated, these individuals often present as stating that the S/M lifestyle was problematic for them and they had to give it up. It is important to note that some individuals give up specific sexual behaviors for a variety of reasons and that is not necessarily contraindicated. Nevertheless, denial of one’s sexual orientation is usually considered to be problematic. Individuals who present with this concern should be seen as in a similar state as homosexuals going through the “coming out” process.
-
Can you make these desires go away? Some S/M people yearn for a more mundane sexual lifestyle and wish to change their sexual orientation. Unfortunately, sexual orientation is either impossible or very difficult to change, as studies of people attempting to change homosexual orientation indicate. It is important to point out that you can help individuals add new behaviors to their sexual pattern. Thus, you can help an S/M practitioner eroticize non-S/M behaviors, but attempts to uneroticize S/M behavior is rarely, if ever, lasting or successful. There is also an ethical question of whether this is appropriate or not.
Attempts at reassurance and education are occasionally helpful, but most clients seeking to change their sexual orientation will not be satisfied with anything less than rigorous therapeutic intervention. Individuals who present with this problem can be seen as analogous to individuals with egodystonic homosexuality, as described in the Diagnostic and Statistical Manual of Mental Disorders, third edition (1980).
-
The SIM is destroying our relationship. Most couples have at least occasional relationship problems and couples who practice S/M as part of their sexual pattern are no different. It is common for the couple to blame the S/M aspect of the relationship for the problems, but couple therapy often uncovers more mundane causes. In either case, mundane or S/M-oriented causation, traditional couple therapy is often helpful. Knowledge of the S/M subculture is essential for the couple’s therapist to make a meaningful intervention.
It is interesting to note that not all S/M practicing couples are composed of a dominant and submissive partner. Many of the couples experiencing problems are composed of two primarily submissive individuals who take turns playing the dominant role with each other. This obviously can become a problem area over time. A smaller number of couples exists where both partners are primarily dominant, but these tend not to engage in S/M acts with each other.
-
I cannot lead this double life anymore. There are numerous examples among S/M practitioners of discrimination when their sexual behavior became known. People have lost jobs, been disinherited, lost friends, lost custody of a child, etc., due to their S/M behavior. This has led many individuals to be exceedingly secretive about their S/M activities. Use of pseudonyms, post office boxes, and other devices to confer anonymity are common. This can lead to stress and dissatisfaction with the S/M lifestyle. Denial of S/M interests can eventuate in stress and dissatisfaction with the vanilla (the S/M subculture’s adjective for non-S/M) lifestyle.
Even when fear of being found out is not the overriding fear, there are problems with integrating the S/M lifestyle into the everyday world. Some S/M practitioners would like to live their lifestyle 24 hours a day, but cannot due to demands of earning a living or other commitments. That they are not able to live their S/M lifestyle the way they would like is often described by these individuals as being forced to lead a double life.
This problem is often a difficult problem for the individual to work through. Assisting the client in finding a support group, couple therapy, and creative solutions such as working for other S/M practitioners or in nontraditional jobs where more options are available has been helpful.
-
I cannot find a partner. While the author has not seen many of these individuals professionally, this may be the most frequent complaint in the S/M community. With a small number of S/M support groups, few women who openly admit their S/M interests, and the difficulty in finding a partner who has complementary interests in both type and intensity of activities, it would seem reasonable that this problem would be a major issue in the S/M community. On the other hand, this is a general problem that is affecting the entire single population.
It has been the author’s experience that S/M practitioners who complain about the difficulty in finding S/M partners are those who also háve problems finding non-S/M partners. Social skill training has been useful in these cases. It should also be noted that many S/M practitioners have been very successful in “bringing out” partners, taking people who have never been involved in S/M and turning them into enthusiastic practitioners. It is not known if these converts to S/M would continue engaging in the behavior if the original relationship broke up, but there are indications that they do in at least some cases.
-
Is it violence or S/Ml These cases often come to the author’s attention through a legal route. The question arises in relationship to spousal abuse, child abuse, rape, sexual harassment, etc. It has been the author’s experience that S/M practitioners are not interested in pursuing their sexual interests unless their partner is willing. This situation is similar to the distinction between rape and consentual coitus. Nonrapists quickly lose interest in coitus if their partner is unwilling. On the other hand, some S/M participants engage in violent acts, either as part of their S/M interests or in spite of their S/M interests.
In these situations, the most important question is “If the victim (this is usually a criminal case) was becoming sexually aroused by being forced, how would that have affected you?” Rapists, sociopaths, etc. report that if the victim was enjoying or aroused by the assault, it would negatively affect their arousal or have no effect. Informal questioning of S/M practitioners suggests that if the person was not enjoying the act, they would stop. This is then a major difference between these two groups. The distinction is important clinically. If the person committing antisocial acts is truly antisocial, then the prognosis is not good as successful intervention is rare. If the person is a poorly socialized S/M practitioner, then we have several options. Socialization has been an important treatment goal that has helped the individual refrain from antisocial acts in the future.
In the present author’s experience, the S/M practitioner rarely commits these violent acts. When an S/M practitioner is involved in violent acts, it is usually seen as separate from the S/M component of their life.
Summary
While there is a paucity of data concerning the psychological problems of S/M practitioners, some preliminary data has been presented. S/M practitioners have not been shown to have any particular psychiatric problems or even any unique problems associated with their activities that interfere with daily functioning. There is no scientific basis to deny S/M practitioners child custody, adoption opportunities, any job, security clearances, or any other right or privilege in this society.
Resources
Support groups for S/M practitioners come in many varied forms. There are general groups, homosexual groups, groups for dominant men and submissive women, groups for dominant women and submissive men, groups around a specific activity which may include both S/M and non-S/M practitioners (e.g., piercing), women’s groups, men’s groups, etc. These groups organize and dissipate regularly, so no listing would stay current for long. Below, two groups are listed. They are the two oldest S/M groups and both do not limit their membership by orientation or other criteria except an interest in S/M. Both have at least contacts in other cities, if not actual group meetings. Both publish information and magazines with useful information for the S/M practitioner. They are:
The Eulenspeigel Society
The Society of Janus
P.0. Box 2783 New York, NY 10163
P.O. Box 6794
San Francisco, CA 94101
References
Annon, J. (1974/1975). The behavioral treatment of sexual problems (Vol. 1 & 2). Honolulu: Enabling Systems, Inc.
Breslow, N., Evans, L., & Langley, J. (1985). On the prevalence and roles of females in the sadomasochistic subculture: Report of an empirical study. Archives of Sexual Behavior, 14, 303–317.
Breslow, N., Evans, L., & Langley, J. (1986). Comparisons among heterosexual, bisexual, and homosexual male sadomasochists. Journal of Homosexuality, 13{ 1), 83–107.
Bullough, V., & Bullough, B. (1977). Sin, sickness, and sanity. New York: Meridian Books.
Diagnostic and statistical manual of mental disorders (1980). Washington, D.C.: American Psychiatric Association.
Ellis, H. (1936). Love and pain. In Studies in the psychology of sex (Vol. 1). New York: Random House. (Original work published, 1903)
Ford, C. S., & Beach, F. A. (1951). Patterns of sexual behavior. Scranton, Pennsylvania: Harper & Brothers.
Gebhard, P. (1976). Fetishism and sadomasochism. In M. Weinberg (ed.), Sex research. New York: Oxford University Press.
Gosselin, C., & Wilson, G. (1980). Sexual variations. New York: Simon and Schuster.
Kinsey, A. C., Pomeroy, W. B., Martin, C. E., & Gebhard, P. H. (1953). Sexual behavior in the human female. Philadelphia: W. B. Saunders Company.
Kokkoka (1965). The koka shastra (A. Comfort, Trans.). New York: Stein & Day. (Originally written 1150)
Krafft-Ebing, R. von (1965). Psychopathia sexualis: A medico-forensic study (F. S. Klaf, trans.). New York: Bell Publishing Company, Inc. (Original work published 1886)
Lee, J. (1979). The social organization of risk. Alternative Lifestyles, 2, 69–100.
Levitt, E. E. (1971). Sadomasochism. Sexual Behavior, September, 69–80.
Maslow, A. (1966). Self-esteem (dominance-feeling) and sexuality in women. In M. De Martino (ed.), Sexual behavior and personality characteristics. New York: Grove Press, Inc. Originally published 1963). (The article was originally published in 1942 in Journal of Social Psychology, 16, 259–294.)
McCary, J. (1973). Human sexuality (2nd ed.). New York: Van Nostrand Reinhold Company. (Originally published, 1967)
Míale, J. P. (1986). An initial study of nonclinical practitioners of sexual sadomasochism. Unpublished doctoral dissertation, the Professional School of Psychological Studies, San Diego.
Moser, C. (1979). An exploratory-descriptive study of a self-defined SIM (sadomasochistic) sample. Unpublished doctoral dissertation, Institute for Advanced Study of Human Sexuality, San Francisco.
Nefzawi, S. (1964). The perfumed garden (R. Burton, trans.; A. H. Walton, ed.). New York: G. P. Putnam’s Sons. (Originally written 1400 A.D.)
Panken, S. (1973). The joy of suffering. New York: Jason Aronson, Inc.
Reik, T. (1976). Masochism in sex and society. (Originally titled Masochism in modem man; M. Beigel and G. Kurth, trans.) New York: Pyramid Books, 1976. (Originally published 1941)
Schad-Somers, S. P. (1982). Sadomasochism. New York: Human Sciences Press, Inc.
Spengler, A. (1977). Manifest sadomasochism of males: Results of an empirical study. Archives of Sexual Behavior, 6, 441–456.
Stekel, W. (1953). Sadism and masochism (2 Vols., L. Brink, trans.). New York: Liveright Publishing Corporation. (Originally published 1929)
Thorpe, L., & Katz, B. (1948). The psychology of abnormal behavior. New York: Ronald Press.
Vatsysayana (1964). Kama sutra. New York: Lancer Books. (Originally written 450 A.D.)
Weinberg, M. S., Williams, C. J., & Moser, C. A. (1984). The social constituents of sadomasochism. Social Problems, 31, 379–389.
Transvestism{5}
Roger E. Peo
Most people take for granted the integration of their sexual anatomy and their feelings of being male or female. A small number of people are not so fortunate. These people are uncomfortable with the gender roles socially forced on them by their sexual anatomy. For them, their sexual anatomy does not allow them to express their inner feelings. They may want to, on some occasions and for a variety of reasons, emulate the other sex.
Transvestism is primarily a male phenomenon although there have been scattered reports of women who cross-dress for fetishistic reasons. In this chapter some historical background on transgender[5] issues will be provided, followed by some generally accepted definitions which lead into a discussion of cross-dressing behaviors. Because cross-dressing is something that men do, and since these men are often in a relationship with a woman, the woman’s situation is discussed. Lastly, relationship issues that arise as a result of the man’s need to wear women’s clothing are covered. Specifically excluded from this chapter are the situations created by genetic and hormonal abnormalities.[6]
In each section clinical and behavioral perspectives are described followed by a description of typical problems that can be presented to the clinician together with some suggested treatment modalities.
Historical Perspective
Transvestism is not a recent phenomenon. From a historical and cultural perspective, men have dressed in women’s clothing as far back as there are records. In several American Indian cultures, there are references to the berdache, a man who dresses as a woman and performs women’s tasks in the tribe (Ford & Beach, 1951). Sometimes such a man was believed to have supernatural powers and became a shaman or very powerful priest. Even earlier accounts can be found in Greek and Roman myths. There is a goddess, Venus Castina, who is said to represent the souls of women “locked up in male bodies” (Bulliet, 1928).
Over the course of time, several different terms for cross-dressing have been used. In the mid-1800s Karl Ulrichs coined the term uranism which linked homosexual behaviors with cross-dressing (Hirschfeld, 1948). Uranism was not used extensively and was replaced by transvestism devised by Hirschfeld. Somewhat later, Havelock Ellis used the term eonism which he derived from the life of Chevalier d’Eon who is reputed to have dressed in women’s clothing for the purpose of spying for Louis XV. Many other historical records exist of men dressing (or being dressed) in women’s clothing for a variety of reasons. The records are not clear about any sexual aspects of such cross-dressing.
Magnus Hirschfeld and Havelock Ellis studied cross-dressing extensively. Both saw it as a variant of homosexual behavior and associated sexual arousal with it. In 1950, Cauldwell devised the term transsexualism which was popularized in 1953 by Dr. Harry Benjamin who used it in a lecture at the New York Academy of Medicine. Dr. Benjamin saw transsexualism as very different from transvestism (Benjamin, 1966).
With that brief historical perspective it is easy to understand that there have also been many colloquial terms used to describe crossdressing males. Many of these terms intermingle homosexual behavior with that of transvestism although that is clinically incorrect. Perhaps the most common term is “drag queen.” The term “drag” is used to describe a man dressing in women’s clothes as a misogynistic parody of women. In homosexual subcultures a “queen” is usually an effeminate homosexual male. Thus, a drag queen is a cross-dressing homosexual male and often what someone thinks of when the term transvestite is used. However, most cross-dressing males are heterosexual and quite invisible to general society.
Cross-dressing Behaviors
The clinical reasons why some males are driven to cross-dress are unknown. There has been a great deal of research and many theories have been advanced (Benjamin, 1966; Ellis, 1936; Green & Money, 1969; Gosselin & Wilson, 1980; Stoller, 1975). The reasons for such behaviors are neither understood nor agreed upon. As clinicians and researchers learned more about the phenomena of transvestism and transsexualism it appeared that there were some fundamental differences in these behaviors. While not definitive, childhood behavior seems to have some value as a predictor (Bullough, V., Bullough B. & Smith, R., 1983).
Cross-dressing can be driven by internal mechanisms or by outward requirements.[7] It is not possible to determine solely by observation what motivates this behavior. Some transvestites say they cross-dress to escape the pressures and expectations of the male role in this society because when they are dressed as a woman, they do not have to act in “masculine” ways (Bullough, V., Bullough, V. & Smith, R., 1983). Some cross-dressers feel they have a feminine side which can only be examined and expressed through crossdressing. To work clinically with cross-dressers (transvestites) it is necessary to distinguish that behavior from transsexualism, for the treatment modalities are usually quite different. The definitions and etiologies which follow are presented in a polar manner to sharply delineate the behaviors. In reality things are not quite so clear cut.
Definitions
To build a foundation for the definitions of transvestism and transsexualism, several other terms have to be defined.
Gender Identity — A person’s internal perception of him/herself as either a man or a woman. Usually it matches the anatomical sex. For example, a person who has male genitalia usually thinks of himself as a man. It is generally believed that a person’s gender identity is solidly formed by three years of age.
Gender Role — A person’s external behaviors that define her/him to society as a woman or a man. These actions are the socially acceptable behaviors for each sex. In most cases, a person’s gender identity and gender role are the same. That is, a person who thinks of herself as a woman will act in “feminine” ways.
Sexual Partner Choice—This is a person’s selection of partner(s) for sexual interactions. There are four generally accepted categories:[8]
-
Asexual—This person has no sexual partners. He or she may, however, masturbate as means of sexual outlet.
-
Heterosexual—The person almost always chooses persons of the other anatomical sex as a sexual partner.
-
Bisexual—The person chooses persons of either anatomical sex as sexual partners. This choice can be serial or concurrent, and the person may have partners of both sexes in the same time period.
-
Homosexual—The person almost always chooses persons of the same anatomical sex for a partner.
Transsexualism — The term literally means cross-sex and while it appears to share some behaviors with transvestism there are significant differences. It appears that there are about equal numbers of male-to-female and female-to-male transsexuals although the overall incidence is much lower than transvestism. In the United States several thousand people have undergone genital reassignment surgery to change their external genitalia to that of the other sex (insofar as possible). This surgery does not make the person a genetic or reproductively functioning member of the other sex. Other transsexuals live full-time in the gender role of choice but do not undergo the genital reassignment surgeiy.
Transsexuals are often very unhappy with their sexual anatomy and may go to extreme lengths to obtain genital reassignment surgery. Self-mutilation and suicide attempts are not uncommon. Drug and/or alcohol abuse may be used to escape the feelings. Opposite sex hormones will often be used if available, either with or without medical supervision.
Transvestism — The word literally means cross-dressing (which is often preferred by transvestites as a less clinical term). Transvestism has been characterized as obsessive-compulsive behavior and used to describe any behavior in which a male becomes sexually
aroused from wearing clothing that is socially reserved for women. It has been used to portray any behavior from wearing a single article of women’s clothing to completely dressing as a woman. Various researchers have estimated that 1% to 5% of the males in the United States are cross-dressers. Because of the social stigma attached to such behaviors, no definitive estimate has ever been made.
Cross-dressing is NOT LINKED to sexual partner choice. The assumption is often made that a male who wears women’s clothing and emulates feminine behaviors must want a male for a sexual partner. Gender identity and sexual partner choice are different behaviors. Any combination of the two is possible.
The generally accepted clinical indications of transvestism are:
-
Start of cross-dressing behavior after five years of age and perhaps not until puberty or later. Early cross-dressing experiences may be linked to sexual or sensual experiences with women’s clothing.
-
Sexual arousal from dressing in articles of women’s clothing which may diminish with age or frequency of dressing. In the early years the male may masturbate while wearing the women’s clothing. Such masturbation may continue into adulthood, even when there is a steady sexual relationship with another person. Sexual fantasies may include being female or living full-time as a woman.
-
Gender identity is usually masculine although there are periods that he may describe himself as “feeling female.” Some observers report a change in the male’s behavior and personality when he is cross-dressed.
-
Gender role is usually masculine except when fully cross-dressed and then he will often attempt to emulate feminine behaviors, mannerisms, and voice.
-
Sexual partner choice is usually heterosexual although there are instances of both bisexual and homosexual partner choices.
A few transvestites will experiment with female hormones if they are available. Others will have electrolysis for beard removal and/or shave off their body hair. There are only a few males who are polished enough in feminine behaviors and appearance to be able to pass successfully as a woman in public.
For both transvestism and transsexuality there are no known hormonal, genetic, or physical reasons for the condition. The definitions above give an abbreviated insight into these behaviors.[9]
Clinical Treatment of the Cross-Dresser
The initial and early counseling sessions are best done without the client being cross-dressed.[10] This has the advantage that the clinician can see the man in his usual state and the man’s anxiety will be less since he did not have to “run the gauntlet” while cross-dressed. In later sessions it may be appropriate for the client to cross-dress but this should usually be done at the clinician’s office rather than having the client arrive cross-dressed. Except in very special circumstances the client should change back to his male clothes before leaving the office.
Whenever the client presents himself[11] to the therapist it is imperative that the clinician take a thorough sex and medical history.[12],[13] By the time the average transgendered person arrives at the therapist’s office, he often has done much research on the phenomenon and has talked to other people in similar situations. As a result of this investigation the client can be more informed on his situation than the therapist. This can pose a problem for the therapist because the client knows what to say, whether or not it is true, in order to gain his ends. Because of this extensive investigation, the client may also “modify” past experiences to be more in line with what he thinks is happening to him in the present. For example, he may “remember” extensive cross-gender behavior at a very young age and “forget” the sexual arousal experiences that he has had.
Regardless of the data gathered from this history taking, it is important not to make an early diagnosis of transvestism or transsexualism. The treatment should probably always proceed as if the client were transvestitic even when transsexualism is suspected.[14] Such treatment is safer for the client because irreversible body alterations are avoided.
It is important to determine why the person has come to see the therapist. There are two broad categories — out of choice or because the client was coerced. The client who comes from personal choice will have a better chance of resolving the cross-dressing issues than one who has been coerced into coming, often by a partner/parent who has sent him to the clinician “to be cured.”
There can be hidden contributing factors which may not come out when taking the initial history. For example, some transvestites may be children of alcoholics or may have been victims of child abuse. In addition, clients may be either alcohol or drug abusers themselves. It is also possible that cross-dressing is being used as an escape from childhood or adult problems. Any of these situations is beyond the scope of this chapter but poses real consequences for the therapeutic outcome.
From birth, usually depending on observed anatomical sex, a person is programmed into the socially acceptable sexual behaviors for that sex. He or she is usually treated in different ways and soon learns what is appropriate (and inappropriate) behavior for the assigned sex. This programming quickly becomes ingrained and subconscious. When someone meets a person who appears to be one sex but behaves in ways that seem more appropriate to the other sex there can be confusion or fear because the behaviors do not match what is expected. This uncertainty and confusion may result in anger or aggression toward such an individual.
In this society there is more concern about males cross-dressed as females than the reverse situation. Cross-dressing is a problem because it goes against socially established behaviors for men and women. Transvestites are not hazardous to other people. They are not exhibitionists, voyeurs, or child molesters. Few laws exist that specifically prohibit cross-dressing behavior. A cross-dressed male’s legal problems often fall into the category of disorderly conduct or some similar catch-all statute. For those who encounter a transvestite the threat is more perceived than real, except for someone who is in an intimate relationship with a transgendered person. Then steps have to be taken to reach some compromise or the relationship can be destroyed.
Since the transvestite is not dangerous to other people, the preferred clinical treatment is to help the man find ways to engage in cross-dressing activities that are not damaging to any relationship he may be in. The harm to the individual is often guilt and fear. Because the behavior is deeply ingrained and often obsessive, the person is helpless to stop the behavior. The therapeutic approaches suggested below address ways in which the clinician can help the client understand his behavior and integrate it into his lifestyle in harmless ways.
Therapy involving sexual situations carries with it some special problems. A clinician can have biases about sexual behaviors that he/she is not even aware of and/or has not come to terms with. This is particularly true when dealing with a transgendered client. Such a client presents situations that are contrary to “traditional” roles and behaviors. A difficulty that some therapists share with the general public is that cross-dressing behaviors are seen as inherently bad and so must be eliminated. If the therapist’s goal is elimination of such behavior, the therapeutic outcome can be less than favorable.
Transvestism is so solidly fixed in a man’s personality that it is usually neither desirable nor possible to eradicate it. A myth the general public has is that if the cross-dresser uses “enough willpower” he will be able to stop cross-dressing. Many forms of therapy have failed to achieve a lasting cessation although the behavior may temporarily stop, especially if the person is under pressure to stop.
Another situation is more common. Often the client is the first transgendered person the therapist has ever encountered. There is a fascination with this new experience. The client becomes a learning experience for the therapist. While this is not necessarily bad, it can have consequences in the therapy because the client has the opportunity to “steer” the therapist toward outcomes that may not be in the client’s best interests.
While the details of therapy cannot be dealt with here, some general approaches are outlined. It is important that the client believes that his behavior is acceptable to the therapist. The therapist may be the first person who has not censured his behavior outright. It is often useful to determine how the client would handle his crossdressing if there were no constraints on his behavior or appearance. The average cross-dresser often has only a minimal grasp of what it really means to be a woman in this society. It can be useful to have the client investigate the woman’s role in society. Guided imagery is often a helpful approach for such explorations.
Depending on the client’s total situation it may be desirable to “give permission” for him to cross-dress more frequently and/or more completely. With this permission are risks. A client may enter what is called in the subculture a “blow-out phase.” This means that he will cross-dress as often as possible and spend as much money as possible on women’s clothing. If he is living alone this may be tolerated. If he is living with his wife or girlfriend, a tremendous strain can be put on the relationship. This phase can be as short as a few months or as long as several years. In some cases the intensity of cross-dressing desire may never diminish. There is a small possibility that the client may decide to live full-time as a woman.
Another aspect of cross-dressing is the intense desire to go out in public dressed as a woman. While some men can carry this off quite convincingly, most cannot. Men and women have different body language. Most men do not change this when cross-dressed. The average man’s size and body structure creates problems in “passing,” but a larger portion is due to the man’s desire to go out inappropriately dressed. For example, he may want to go to a shopping mall dressed in a mini skirt, 5” spike heels, and seamed black stockings. The other time a cross-dresser will often go out dressed as a woman is at times when a woman would probably never go out. This might be at 11:00 p.m. to mail a letter. Also he may go to inappropriate píaces such as a singles bar. All of these situations can create serious problems. The therapist should strongly dissuade him from these activities and suggest alternatives such as joining a transvestite club that sponsors safe social situations. The therapist can also offer to write a letter stating that the cross-dresser is under her/his care and that he is neither dangerous to himself or others.
The therapeutic thrust is to assist the client in integrating the cross-dressing with the rest of his life. Techniques that rely on extensive investigation of the client’s past are not very useful with this dysfunction, because they may be hindered by client “alterations.” Any techniques that the therapist has familiarity with and which allow dynamic interaction with the client are more useful. Hypnosis; dream interpretation; working with artists’ media such as paints, crayons, markers, etc.; gestalt techniques; videotaping and playback; and psychodrama have all proven useful. The goal is to help the client understand what benefits he derives from the crossdressing together with helping him find ways to integrate the crossdressing into his life without damaging other portions and relationships. He has to control it rather than it controlling him. For transvestites there is no magic solution or right answer; each case presents a unique situation and requires a unique solution.
Women Partners of Transvestites
The cross-dresser is often quite inexperienced with women. Often a cross-dresser enters into a relationship with a woman because he hopes that having an intimate and committed relationship with a woman will somehow eliminate his desire to cross-dress. This idea can carry over to the woman who may think that she can, somehow, help him to get over this desire to cross-dress. Often the exact opposite occurs. The cross-dresser is now exposed on a regular basis to a woman’s dressing and undressing which becomes a constant reminder that he would like to be wearing those clothes. If she is not aware of his need, the pressures of keeping those needs from her will create stresses in the relationship. If she does know, there is a likelihood that he may pressure her to let him dress more frequently, creating different stresses.
Perhaps one of the strongest misconceptions about women who are in a relationship with a transvestite is that they are unique. The remarkable thing about such women is that they are so unremarkable. They are neither self-destructive nor do they have “lesbian tendencies”; neither are they super women. These women fall into two categories —those who knew about their partner’s cross-dressing before entering a committed relationship and those who found out after committing to the relationship. For both categories, the women seem to have some common characteristics —they are deeply in love with their partner and they are often very supportive, putting his needs ahead of their own (Peo, 1984). In some ways these women are like the succorer described by Stoller (1967), “a woman who supports cross-dressing with sympathy.... Their most conspicuous quality is a pronounced need to succor other creatures.”
Whether or not the woman knew of her partner’s cross-dressing before committing to the relationship, several emotions and reactions seem to be common. The most typicaL is that she is somehow at fault for his cross-dressing. Perhaps she is not attractive enough, sensitive enough, etc. This leads to deep-seated feelings of guilt. Closely following this is doubting her own sexuality and feelings of self-worth. She may wonder if she is a lesbian. She may think that she is “not good enough” to attract a “real” man.
Along with these personal problems will come her need to deal with his cross-dressing before and/or during their sexual relations. Because cross-dressing can be associated with his sexual arousal, the woman has to cope with her partner’s arousal when it is not arousing for her and, in fact, has the likelihood of decreasing her sexual arousal. She may feel that he is only aroused by the clothing and not by her which can lead to other sexual problems.
Somewhere in her emotions is fear. She will be afraid that someone will find out and concerned about what that discovery could do to her, her children, her husband, his job, their friends, and social life, etc. She will worry about the children discovering his crossdressing and what this could do to them. If her partner goes out cross-dressed, she will be afraid that he will be caught and arrested. Because cross-dressing is socially unacceptable, she is often hesitant to discuss it with her close friends, which further isolates her. There are no books for her to read and few ways to get information about her situation.
From the clinician’s point of view some other observations are pertinent. The average woman partner of a transvestite will often be in her mid-30s or somewhat older. She will probably have less formal education than her partner and will have been in the relationship long enough to have deep emotional ties to him. If they are married and even if she is in the work force she is most likely to be economically dependent on him. Women of this age will have experienced a unique social environment during her life. She is a “transition” woman, that is she has lived through the birth of women’s liberation, yet, her early upbringing may have been quite traditional. This significant social change may leave her unsure how to react toward her partner and yet have her needs met.
Clinical Treatment of the Woman Partner
In the same manner as with the cross-dresser, a complete medical and sex history should be taken from her.[15] During early sessions, it is very important to see the woman alone. It is likely that she has come because her partner has urged her to come. However, having her partner in the room will probably inhibit her responses. The therapist has to assure her that s/he is supportive of her. Only after gaining her trust and confidence is it appropriate for them to be in a joint therapy session.
The woman’s concerns can be divided into three categories— issues of self, relationship issues, and social issues. Immediate attention should be given to supporting her self-image. Without this support, her other concerns will be difficult for her to handle.
Her foremost need is for information. She needs to know that she is in no way to blame for her partner’s cross-dressing. It began long before she knew him and is an immutable part of his personality. Further, she needs to know that his behavior will most likely not lead to genital reassignment surgery, although at times it may seem that he wants to spend all his time cross-dressed. One wife made the insightful observation that her husband was much like a teen-age girl who constantly experiments with makeup and clothes, perhaps to the exclusion of all else.
Along with the above support, she needs to understand that she is OK. The woman is as prey to myths about cross-dressing as the rest of society. Her sexuality is often threatened. She may think she is a lesbian because she loves a man who sometimes likes to emulate a woman, especially in sexual situations. If she is typical, she has never examined her feelings about homosexuality, either for herself or for her partner. It is important to examine social (gender) roles and to see how they can generate homophobic reactions.[16]
In addition, she may have a lot of fears that have been generated by information her partner has given her. Often a well-meaning man will give the woman publications from the subculture. Many of these contain a great deal of fantasy on subjects such as forced cross-dressing and living full-time as a woman. Such articles often increase her fears.
Relationship issues fall into two categories; those felt by the woman and those that influence interactions within the couple. The latter will be left for the section on couple counseling. In our society, the woman is often seen as the one who is responsible for the care and nurturing of a relationship. The woman’s early upbringing can generate guilt. Women in the age bracket most frequently encountered often have been brought up to believe that it is their responsibility to make their partner happy. Thus, she has the task of “making things work.” She may also feel that everything that goes on in the relationship is a reflection on her.
Probably the most difficult thing for her to accept is that he will never be “cured” of this need. If she decides to stay in the relationship, she has to accommodate his behavior in some way. This can range from total participation in all facets of the cross-dressing (buying clothes and/or accompanying him on public excursions while cross-dressed) to complete detachment (never seeing him cross-dressed, etc.). Where she ends up on this spectrum is her individual choice but, wherever it is, she still has to accept the fact that he is a cross-dresser.
In the process of finding how to cope with his cross-dressing, she will try different things. While these may be acceptable to her partner, she may find that she cannot deal with the situations or emotions created during these trials. Because she has no way of predicting how she may feel, she needs to have the therapist’s support in stopping or withdrawing from given situations. This withdrawal does not mean that she is less understanding of her partner, but simply that some of these situations are not acceptable to her or do not meet her needs. Many women neither enjoy nor encourage their partner’s cross-dressing. While they do not blame themselves for his behavior neither do they wish to support it or participate in it.
It is necessary to help her negotiate with her partner on issues such as when he can cross-dress, telling parents or close friends, etc. The key is security —hers and the family. Cross-dressing carries heavy social approbation which may cause significant problems (such as loss of employment) if discovered. Disclosing the crossdressing should be done only on the basis of need.[17] If not telling a person can have serious relationship consequences then disclosure is probably the best choice. Such disclosure should be done slowly and gently. The person should be told verbally, perhaps augmented with photographs. Actually seeing the man cross-dressed is probably going to create problems because most persons have difficulty dealing with cross-dressing.
One of the woman’s greatest concerns is for any children living at home —how to balance her partner’s needs and theirs. While there are no studies, the general consensus of wives and professionals is that young children should not be told. Later, as teenagers or older, it may be appropriate to discuss it. This, of course, puts restrictions on when the man can cross-dress.
She may feel that she cannot talk to her partner about her feelings for fear that he will neither understand nor be supportive. Also, he may take her comments as criticism of his behavior which can drive them further apart. There are national and local transgender support groups that have groups for wives and partners of transgendered persons.[18] In such groups she may be able to find support by talking to women who have experienced situations similar to hers.
With all the problems created by a cross-dressing partner, it seems unusual that a woman would choose to stay in such a relationship. There are women who rate their marriages as happy, yet say their husband’s cross-dressing is distasteful to them. What appears to be true about such relationships is that other aspects of the overall relationship counterbalance these problems (Peo, 1984). Such women feel that their husband could have worse traits such as wife abuser, alcoholic, compulsive gambler, etc. Closely related to this happiness is the woman’s self-esteem. Those women with high self-esteem generally report being able to cope more satisfactorily with their partner’s cross-dressing than women with lower self-esteem (Bullough, V. L. & Weinberg, T. S., 1986).
It may turn out that the woman simply cannot deal with the crossdressing issues. They may cut too deeply at her self-image and/or the constant stress of keeping this secret may be too great. As a result, she may want to leave the relationship, yet, she may be economically dependent on her partner and/or emotionally attached to him. There are often considerations of children and social explanations for the marriage breakup to be dealt with. Supporting her in this situation and helping her find the right path is only peripherally related to cross-dressing and can be dealt with using more usual counseling methods.
Clinical Treatment of the Couple
When counseling the couple,[19] the most important contribution the clinician can make is the establishment of clear communication within the relationship. Cross-dressing influences may intimidate areas of a relationship. Because of fear of misunderstanding and rejection, each person may be very reluctant to say what he or she really feels. This may be more true for the woman than the man. Regardless of the apparent egalitarianism of the relationship, there is usually a power imbalance—with the woman having less power.
The therapeutic environment should not be used to force the woman to accept her partner’s cross-dressing anymore than it should be used to force the man to stop cross-dressing. The therapist has to be careful not to focus exclusively on the cross-dressing issues and ignore the woman’s needs. While her needs may seem simple when compared to the unusual needs of the man, they are as important.
During the overall counseling regimen, the partners should be seen individually as well as in joint sessions. Joint sessions work well for resolving relationship issues, while individual sessions are often a better environment for resolving the individual concerns.
Whether the woman learned of her partner’s cross-dressing before their marriage or afterward, the situations above will generally have to be dealt with. One issue that is different is trust. If the husband has kept his cross-dressing a secret from his wife for an extended period of time and then disclosed it, she may feel betrayed and may lose any trust she had in him. She may also wonder what other secrets he has kept from her. Rebuilding her trust in him is the hardest part of the overall situation. It takes a lot of time and sensitivity on the man’s part to achieve this. While loss of trust is probably not an issue if the woman learns before marriage, it is doubtful that either of them truly realizes the extent to which cross-dressing will influence and permeate their relationship.
From the man’s point of view, freedom to cross-dress whenever and wherever he wants is often his primary goal. Allowed free rein, such cross-dressing can expand to fill every available moment. The woman may be willing to accommodate his cross-dressing so long as it does not dominate their entire relationship.
He may want to cross-dress before and/or during lovemaking. She may strongly want to keep the cross-dressing out of the bedroom, or at least restrict its presence. Cross-dressing may totally eliminate any sexual desire on the woman’s part, yet, she may be afraid to say anything. Allowed to progress, such behavior can lead to sexual dysfunctions on the part of the woman.
One problem can be the man’s borrowing of the woman’s clothes. For a woman, her clothes and makeup are an intimate and essential part of her being and sexuality. If her partner uses them, she may feel violated and invaded. Consequently, it is very important for the man to have his own clothing and not borrow the woman’s clothes, even if she seems willing to allow this.
The clinician has to be the mediator. By providing a safe environment the therapist can support each person in stating his or her needs without threatening the other partner. Once these have been described, the clinician can assist the couple in finding solutions that meet each of their needs. The most difficult part of the task is to help the man to learn to be sensitive to the woman’s needs. He has to learn to curb his needs and to be aware that cross-dressing may not sexually arouse her. Typically, there could be an agreement wherein the husband does not cross-dress for lovemaking in exchange for time to cross-dress later. Generally, he has to be willing to control his cross-dressing and be willing to engage in or support activities that the woman enjoys. The clinician has to help the woman cope with the fact that her partner will always have a need to cross-dress and that she has to allow him the freedom to do this within the constraints they have previously negotiated.
Conclusion
Cross-dressing affects more aspects of a person’s life and relationships than almost any other behavior. While such dependencies as alcoholism are extremely damaging to people and relationships, they do not generally bias the person’s sexual identity and relation
ships. Such a pervasive influence is difficult to deal with. The clinician can do much to support the couple and each individual, yet, the outcome is, at best, problematical. Anecdotal evidence from hundreds of cross-dressers seems to indicate that many women are either unaware or unaccepting of a man’s cross-dressing. Often the woman takes the position that it is “his problem” and that the only solution that is acceptable to her is complete cessation of the crossdressing. Since this is usually not possible, the behavior goes underground and indirectly creates other relationship problems.
Relationships which endure this behavior are those in which the woman has high self-esteem and is willing to accept the cross-dressing coupled with the man’s sincere sensitivity to meeting the woman’s needs. This combination is quite rare. While trying not to be pessimistic, obtaining a positive result from counseling will be very difficult to achieve and perhaps can only be achieved if the woman is willing to sacrifice some of her needs in order to obtain harmony in the relationship.
Often the most a clinician can do is to provide support and accurate information while assisting the person or couple in establishing clear communication so that they can find solutions to their unique situation.
References
Ackroyd, P. (1979). Dressing up: Transvestism and drag. New York: Simon & Schuster.
Benjamin, H. (1966). The transsexual phenomenon. New York: Warner Books. Brierly, H. (1979). Transvestism: A handbook with case studies for psychologists, psychiatrists and counsellors. Elmsford, New York: Pergamon Press.
Bulliet, C. J. (1928). Venus castina. New York: Bonanza Books.
Bullough, V., Bullough, B., & Smith, R. W. (1983). A comparative study of
male transvestites, male to female transsexuals and male homosexuals. The Journal of Sex Research, 19:3, pp. 238–257.
Bullough, B., Bullough, V., & Smith, R. W. (1985). Masculinity and femininity in transvestite, transsexual and gay males. Western Journal of Nursing Research, 7:3, pp. 317–322.
Bullough, V. L., & Weinberg, T. S. (1986, November). Alienation and self-image among wives of transvestites. Paper presented at the Annual Meeting of the Society for the Scientific Study of Sex, St. Louis, Missouri.
Bush, P. J. (1980). Drugs, alcohol & sex. New York: Richard Mark Publishers.
Ellis, H. (1936). Studies in the psychology of sex. New York: Random House.
Feinbloom, D. H. (1976). Transvestites and transsexuals. New York: Dell.
Ford, C. S., & Beach, F. A. (1951). Patterns of sexual behavior. New York: Harper & Row.
Gosselin, C., & Wilson, G. (1980). Sexual variations: Fetishism, sadomasochism, transvestism. New York: Simon and Schuster.
Green, R., & Money, J. (1969). Transsexualism and sex reassignment. Baltimore: Johns Hopkins Press.
Hirschfeld, M. (1948). Sexual anomalies. New York: Emerson Books.
Kinsey, A. C., Pomeroy, W. B., & Martin, C. E. (1948). Sexual behavior in the human male. Philadelphia: W. B. Saunders.
Money, J. (1968). Sex errors of the body. Baltimore: Johns Hopkins Press.
Peo, R. E. (1984). Women who relate to male transvestites: A descriptive study. Unpublished doctoral dissertation, the Institute for Advanced Study of Human Sexuality, San Francisco.
Pomeroy, W. B., Flax, C. C., & Wheeler, C. C. (1982). Taking a sex history. New York: The Free Press.
Prince, V. (1976). Understanding cross-dressing. Los Angeles: Chevalier Press.
Stoller, R. J. (1967). Transvestite’s women. American Journal of Psychiatry, 124:3, pp. 333–339.
Stoller, R. J. (1975). Sex and gender, volume II: The transsexual experiment. New York: Jason Aronson.
Stoller, R. J. (1985). Presentations of gender. New Haven: Yale University Press.
Stuart, K. E. (1983). The uninvited dilemma. Lake Oswego, Oregon: Metamorphous Press.
Transsexualism{6}
Sharon B. Satterfield
Definition
Transsexualism is defined by the Diagnostic and Statistical Manual of Mental Disorders (DSM-III-R) of the American Psychiatric Association as:
-
Persistent discomfort and sense of inappropriateness about one’s assigned sex.
-
Persistent preoccupation, for at least two years, with getting rid of one’s primary and secondary sex characteristics and acquiring the sex characteristics of the other sex.
-
The person has reached puberty.
The sense of discomfort and inappropriateness about an individual’s anatomic sex is usually referred to as gender dysphoria. Clinicians working in the field realized quite early that different patients had varying levels of gender dysphoria. The best description of this continuum of gender dysphoria is perhaps that put forth by Harry Benjamin. Benjamin (1966) described a seven-point scale not unlike the Kinsey Scale for homosexuality. Individuals falling on the scale had the following characteristics:
-
This is a “normal” individual with no gender dysphoria.
-
Pseudo transvestite (TV). This is the transvestite usually ranging from strictly heterosexual to strictly homosexual and is defined by showing sporadic cross-dressing, most of which occurs during masturbation and fantasy.
-
Fetishistic TV. This is the transvestite usually ranging from exclusively to mostly heterosexual (Kinsey Scale 0–2). This individual dresses periodically in clothing of the opposite sex, usually wearing garments under male clothing. Transvestites, as described by Benjamin, are almost entirely male.
-
True transvestite (ranging from 0–2 on the Kinsey Scale) often dresses in women’s clothing and may actually live as a female. This individual is heterosexual except when cross-dressed.
-
Nonsurgical transsexual. This person ranges from 1–4 on the Kinsey Scale and cross-dresses, often with insufficient relief of the gender dysphoria from the cross-dressing. The sense of gender discomfort in this individual is present early in life, although not intense, and often increases with age. Other clinicians refer to this entity as secondary transsexualism and find this group to be the most puzzling and difficult individuals because of their ambivalence.
-
True transsexual, moderate. This person ranges between 4 and 6 on the Kinsey Scale (usual to exclusive homosexuality). He or she lives and works as a member of the opposite sex, if possible, but may have tried to adapt to the normal sex roles of the biological gender and may have married and had children. Usually surgery is indicated in this individual.
-
True transsexual, intense. This person tends to be exclusively homosexual, as defined by the biological gender, although they see themselves as heterosexual. Their gender discomfort is intense, and they get very little relief from cross-dressing. These individuals are usually clinically evident at an early age and truly believe themselves to be trapped in the wrong body.
The “true transsexual” will likely give an early childhood history of wishing to be a member of the opposite sex, often from earliest memory. Cross-dressing usually begins quite early in life and is usually accompanied by stereotypical cross-gender play and the choice of playmates of the opposite gender. For the biological male, this often involves playing with dolls or playing house, and for the biological female, this usually involves a reluctance to wear dresses or to play with dolls or other sedentary play. Girls typically will seek out rough and tumble play, whereas gender dysphoric boys will avoid it. Usually at some point, the gender dysphoric male is labeled a “sissy” and is often socially ostracized because of this. The gender dysphoric female is likely to be labeled a “tomboy” but is less likely to suffer negative social consequences and may actually be rewarded for this behavior.
The transvestite typically has a later onset of cross-dressing, often at puberty. Cross-dressing is usually fetishistic in nature and is accompanied by sexual arousal to the cross-dressing itself. The transsexual, on the other hand, tends to be more asexual and is so aversive to the genitals that there is often a reluctance to masturbate by touching them. Although they are usually attracted to members of the same biological gender, they see themselves as heterosexual since they themselves are in the wrong body. They may also be homosexual or bisexual. Transvestites may be heterosexual, homosexual, or bisexual but are most likely to be heterosexual. It should be noted that in the mid-thirties, a transvestite is frequently observed to become more gender dysphoric and may actually lose the fetishistic nature of masturbation. It is not uncommon that individuals previously diagnosed as transvestite later in life request sex reassignment surgery and may be appropriate for it.
Egodystonic Homosexual
It should be pointed out that individuals suffering from genetic or hormonal abnormalities demonstrated by an ambiguous genitalia should first be treated by procedures commonly accepted for those medical conditions. It is likely that patients with Klinefelter’s Syndrome will have a higher incidence of gender dysphoria than the normal population, and may be candidates for a gender treatment program, after appropriate medical treatment. Psychological conditions which are commonly confused with transsexualism include schizophrenia, multiple personality disorder, and dissociative conditions. Occasionally, a patient who has been sexually abused will consciously decide to be a member of the opposite gender in an attempt to avoid sexual abuse in the future (Satterfield, 1984). This usually occurs in females. Males with a very poor self-image have been misdiagnosed as transsexual because they feel that their passivity and lack of stereotyped male behavior is inconsistent with them living as a male. All attempts should be made to rehabilitate patients with psychiatric diagnoses by commonly accepted therapeutic procedures. It should be noted, however, that gender dysphoric individuals may also have a psychiatric condition. Many transsexuals have previously been labeled either schizophrenic or manic depressive. These diagnoses do not preclude the diagnosis of transsexualism or, in certain circumstances, the possibility of hormonal or surgical sex reassignment.
Minimum Standards of Care
The Harry Benjamin International Gender Dysphoria Association, Inc., an international group of professionals committed to the treatment of gender dysphoria, have drafted minimal standards of care recommended for hormonal and surgical sex reassignment of gender dysphoric individuals (Walker, Berger, Green, Laub, Reynolds, & Wollman, 1981).
Briefly, the Standards of Care are considered to be minimal guidelines for hormonal or sex reassignment, not a clinical draft of how to treat the transsexual patient. The burden of responsibility for the decision of recommending an applicant for sex reassignment is placed on the clinical behavioral scientist, who is defined by a possession of a professional or academic degree in a behavioral science. These standards make it clear that the mere possession of a degree does not qualify a person sufficiently to conduct psychotherapy, counseling, or diagnosis of gender identity problems. It is recommended that this person, in addition, should have proven competence in general psychotherapy, sex therapy, and gender counseling, as demonstrated by a license or national certification in one’s field and additional documented training and certification in sex therapy, with a specialization in the diagnosis and treatment of gender identity disorders. Diagnostic evidence for transsexualism requires that the clinical behavioral scientist “have knowledge independent of the patient’s verbal claim that the dysphoria, discomfort, sense of inappropriateness, and wish to be rid of one’s genitals have existed for at least two years” (Walker et al., p. 8). The clinician must obtain this evidence by previous records from other clinicians or interviewing friends or family of the patient, although it is acknowledged that at some point he or she must depend to some extent on the history given by the patient.
The following standards are recommended prior to the initiation of hormonal sex assignment.
-
The patient must demonstrate that the sense of discomfort with the self, and the urge to be rid of the self and genitalia should have existed for two years.
-
The patient must be known to a clinical behavioral scientist for at least three months and that clinical behavioral scientist must endorse the patient’s request for hormone therapy.
-
The patient receiving testosterone should receive a complete physical examination which includes but is not limited to the measurement of SGPT. Patients receiving estrogen should have SGPT, bilirubin, triglycerides, and fasting glucose measured (Walker et al., p. 7–9).
Prior to genital or breast reassignment, the following criteria should be met:
-
The patient must demonstrate the sense of discomfort with the self and an urge to be rid of genitalia to have been present for at least two years.
-
The patient must be known to a clinical behavioral scientist for at least six months in a psychotherapeutic relationship and that clinical behavioral scientist must endorse the patient’s request for genital’Surgical sex reassignment.
-
The patient must be evaluated at least once by a clinical behavioral scientist other than the clinical behavioral scientist specified above and this person must also endorse the request for genital sex reassignment. At least one of the clinical behavioral scientists making the recommendation for genital sex reassignment must be a doctoral-level clinical behavioral scientist.
-
The patient must have been living successfully full-time in the genetically other sex role for at least one year. This included living and working and being known and recognized as a person of the other sex role. A physical examination including urological examination should be performed.
-
During and after all services are provided, the patient’s right to privacy should be honored. The patient should be charged only the appropriate and customary fees for these services (Walker et al., p. 9–10).
The Standards of Care have been made necessary by the fact that “surgery on demand” has been available in some parts of the world and, in fact, some parts of the United States. It has been demonstrated in the literature and by many anecdotes that there are situations in which patients have made impulsive decisions for sex reassignment surgery which they later regret. Because of the irreversible nature of both hormonal and surgical sex reassignment, it is extremely important that the patient first receive informed consent and be acquainted with all the side effects of treatment, some of which are considered life-threatening. For instance, any physician who prescribes hormonal medication to a person for the purpose of sex reassignment should inform the patient of negative complications which may arise, such as thrombophlebitis, increased blood pressure, liver damage, and hepatic tumors. The physician is then also responsible for monitoring relevant blood chemistries and performing physical examinations. The physician should also inform the patient of irreversible consequences of hormones. These may include infertility, hair growth, voice deepening, and clitoral enlargement in the female-to-male patient and infertility and breast growth in the male-to-female patient. It should also be made clear that there have not been controlled studies done on large numbers of transsexuals on hormonal medication and that the medical profession may not be aware of all the complications which may arise.
Several lawsuits around the country against physicians who have prescribed hormonal or surgical sex reassignment have actually led to the closing of gender clinics. Ironically, when, in medicine in general, the patient is better informed and given more control of decisions for his or her body, the physician appears to be held even more responsible for the decisions the patient makes. It should be noted that most transsexuals in over 50 follow-up studies have said very clearly that they have no regrets about surgery and by far the majority of follow-up studies show positive results in this population (Lothstein, 1982).
A follow-up of 27 patients from the University of Minnesota has demonstrated significant improvement in vocational, social, and psychological adjustment (Satterfield, 1983). This improvement correlates positively with the length of time since surgery and to the degree of gender dysphoria prior to surgery. There are no correlations between the satisfactory outcome following surgery and preoperative social or psychological adjustment. From this data, we find that we need to carefully examine the criteria used to assess the transsexual and to rely on the degree of gender dysphoria and the overall emotional stability of the patient, as well as the ability to live successfully in the role. Chemical dependency has been found in the Minnesota sample to lead to a very poor prognosis; therefore, it is recommended that individuals who are chemically dependent be given an additional year of sobriety before having the usual Standards of Care applied.
Comprehensive Treatment Program
Gender dysphoric individuals have usually suffered for many years, feeling a sense of alienation from society because they believe themselves to have a unique problem. When, through reading or contact with other gender dysphoric persons they discover that they are not alone, they usually have an initial sense of relief but still continue to hide their gender dysphoria from persons, family members, and other persons with whom they have a close relationship. This ultimately leads to compartmentalization of their lives and obvious problems with intimacy, since they are unable to share their greatest secret.
Most transsexuals report previous bouts of depression due to their sense of alienation, which becomes one of the greatest diagnostic dilemmas for the clinician working with them. It is necessary to distinguish whether this depression is a reaction to discrimination they have received, the sense of alienation which they feel, or is more endogenous and likely to cause problems after appropriate treatment for the gender dysphoria. Group therapy is initially recommended lor transgender individuals for the following reasons:
-
All of them at some point in their lives suffer a sense of uniqueness and need to meet other individuals with the same problems.
-
Transsexuals usually present with the obsession of obtaining sex reassignment surgery immediately. This is most adequately confronted and alleviated by being part of a group with other individuals who have successfully struggled with this demand.
-
Transgender individuals are likely to show a high incidence of depression, psychosomatic complaints, and chemical dependency. This appears in clinical experience with more than 300 transsexuals.
-
Therapy groups often function as a support system. It is important that transgender individuals develop a social network, which is often possible only after receiving an emotional support offered in a group situation.
Evaluation of the gender dysphoric person should include an extensive period of history-taking, which includes very specific details of early childhood, sexual activity, and interpersonal relationships. Very careful assessment of chemical problems and legal problems should also be attempted. The clinician should not rely on the word of the patient alone, but should attempt to get corroborating evidence by interviewing family members, previous friends, and obtaining past medical and psychiatric records. Extensive psychometric testing is recommended which includes a personality profile such as the MMPI, Sexual Attitude and Behavior Survey, a BEM Sex Role Inventory, and an assessment of self-concept.
It is recommended that the first therapeutic situation be that of a group of other transgender individuals focusing on enabling the patient to articulate exactly what the feelings of gender dysphoria are. It is useful to present the patient with several hypothetical situations, particularly those which would involve not having the opportunity to have sex reassignment surgery, and what other options might be explored. It is important to present the patient with the reality that nothing can make them completely male or female. In fact, the surgery has its limitations and complications but can be useful for some individuals. The purpose of psychotherapy is to integrate all portions of the personality and have the patients develop a sense of acceptance of the gender dysphoria. Only at this point can one assess whether hormonal or surgical sex reassignment will be required. Lothstein reports a certain degree of success in reversal of gender dysphoric patients with psychotherapy (Lothstein, Levine, Leslie et al., 1981). This is likely to be a minority of patients; however, it is important, particularly for those in Harry Benjamin’s Category 4.
There will be a certain group of patients who will be judged as not being appropriate candidates either because of the low level of their gender dysphoria or because of contraindications to sex reassignment. The clinician must be aware that to treat these patients means the maintenance of many individuals without the hope of ultimate surgery. This may require years of working with social service workers and other community support people to provide an adequate environment in which the patient is not overtly discriminated against. This is particularly important if the patient should . require institutionalization for any reason.
It is recommended that a weekly group for at least three months’ duration be required of all patients before considering hormonal sex reassignment. Bimonthly or monthly group meetings for an indefinite period may then be required before the patient is judged an adequate candidate for sex reassignment. The most important time for support for the patient is usually when the actual cross-living commences. This is the actual sex reassignment and is usually a period of high-anxiety and requires the greatest emotional support. If a period of one to two years of cross-living goes well, surgical sex reassignment is usually seen only as incidental by all parties involved.
The timing of hormonal sex reassignment varies a great deal from one individual to another and is definitely not necessary in all cases. Because of serious side effects, it should be considered only for specific reasons, such as the growth of facial hair in female-to-male transsexuals or the development of breasts in the male-to-female. For the male-to-female transsexual, usually oral Premarin is prescribed. For the female-to-male, intramuscular Depo-Testryl is recommended. A transsexual usually succeeds in “passing” as a member of the opposite sex through the experience of practice.
Very rarely do hormones make the difference except in the particularly feminine-appearing female-to-male.
Adjunct therapies which are often required for the gender dysphoric patient are family therapy, evaluation of children in the family, sex education, and grooming/makeup classes. Many gender dysphoric individuals will require ongoing individual psychotherapy and possibly medication for an extended period.
Unfortunately, the prognostic indicators for the gender dysphoric individual may be factors over which neither the patient nor the therapist has much control. Walinder, Lundstrom, and Thuwe (1978) have listed significant prognostic factors, such as inappropriate physical build, lack of family support, criminality, inadequacy of self-support, and unstable personality as unfavorable signs. Although gender dysphoric patients have been known to overcome great obstacles with the proper support, the person who is not experiencing improved emotional stability and is not “passing” well two years after beginning to live in the role will present serious therapeutic problems. They do not wish to return to the biological gender, but are aware, at some level, that they will never attain their goal of being a “complete” woman or man.
Summary
This article has presented the currently accepted definition of transsexualism for the purpose of diagnosis, as well as the minimum Standards of Care for hormonal or sex reassignment. A comprehensive treatment program has been outlined which recommends initial group therapy for transgender individuals. Evaluation of such individuals must include extensive history-taking and psychometric testing. The decision to treat with hormones or surgery must be made only after a period of psychotherapy which allows exploration of alternative paths to reversing gender dysphoria. Both hormonal and surgical sex reassignment carry associated risks. It must be recognized that many gender dysphoric individuals, no matter what the treatment modality, may require, in addition, ongoing psychotherapy and/or medication for a long period of time.
References
Benjamin, H. (1966). The transsexual phenomenon. New York: Julian Press.
Lothstein, L. M. (1982). Sex reassignment surgery: Historical, bioethical and theoretical issues. American Journal of Psychiatry, 139, 417–426.
Lothstein, L., Levine, S., Leslie, M., et al. (1981). Expressive psychotherapy with gender dysphoric patients. Archives of General Psychiatry, 38, 924–929.
Satterfield, S. (1983). Long-term follow-up of sex reassignment surgery. Paper presented at 8th International Gender Dysphoria Symposium, the Harry Benjamin International Gender Dysphoria Association, Inc., Bordeaux.
Satterfield, S. (1984). Transsexualism as a flight from the female role. Paper presented at Combined Annual AASECT/SSSS Meeting, Boston, Mass.
Walinder, J., Lundstrom, B., and Thuwe, I. (1978). Prognostic factors in the assessment of male transsexuals for sex reassignment. British Journal of Psychiatry, 132, 16–20.
Walker, P. S., Berger, O. C., Green, R., Laub, D. R., Reynolds, C. L. and Wollman, L. (1981). Standards of care: The hormonal and surgical sex reassignment of gender dysphoric persons. The Harry Benjamin International Gender Dysphoria Association, Inc.
Part III: Coercive Sexually Unusual Expression{7}
There is little question that several of the sexual expressions being defined are sexually unusual are essentially coercive in nature and involve an unwilling recipient of the sexual expression. It is also the case that these sexual behaviors will frequently involve the criminal justice system and other societal social control mechanisms. In Part III we focus on several of those essentially coercive sexually unusual behaviors, including pedophilia, exhibitionism, voyeurism, and the obscene phone caller.
The state of our knowledge and clinical intervention strategies is relatively underdeveloped and wide variation in both occur and are reflected in these chapters. The current conceptual struggle about whether sexually coercive behaviors are a single phenomenon or each a discrete expression is highlighted in the perspectives taken in the first three articles.
The final two companion articles have been included to offer one view on sexually aggressive and/or addictive behavior and a model for intervention. The coercive sexually unusual expressions often have an aggressive and addictive element, and so, too, do some of the noncoercive sexual expressions. It is the case that almost any specific sexual behavior can have aggressive and/or addictive qualities. The model described results in a treatment format with positive outcomes, and provides some contrast to some of the other treatment modalities described in the various chapters in this volume. It is not the only successful intervention, by any means, but is included because it appears to genuinely offer help for those persons who suffer from aggressive and/or addictive sexual behaviors. Good outcomes occur despite the fact that aversive behavioral approaches are used, a treatment strategy that many helping professionals seem to find aversive.
Pedophilia{8}
Edward L. Rowan
A1 is a 35-year-old man with a fantasy triggered by seeing a young girl with long blonde hair or by a magazine or television characterization of the same. He then imagines himself disrobing the girl and touching her hairless pubic area and nipple buds. He may masturbate to this fantasy or use it to become aroused enough to have intercourse with his wife. Acting out the fantasy with his stepdaughter led to his arrest.
Bob is a 43-year-old man who was diagnosed as mentally retarded and grew up in the State School. In community placement after deinstitutionalization he played with two 9-year-old boys in the neighborhood and talked them into “playing doctor” with him. There was mutual genital touching.
Carl is a 40-year-old man with a history of alcoholism and conflicts with his alcoholic wife. His oldest daughter had taken over care of the younger siblings and was his confidante. On one occasion, when drunk, Carl fondled his daughter.
Each of these men may be a “child molester” or have sexually assaulted a child; however, their reasons are clearly quite different. Whether or not each is a “pedophile” is a matter of definition.
Pedophilia is narrowly defined by the Diagnostic and Statistical Manual of the American Psychiatric Association (1980) as one of the paraphilias, or “the act or fantasy of engaging in sexual activity with prepubertal children as the preferred or exclusive method of achieving sexual excitement.” Such a group of offenders comprises only a small part of the universe of child molesters. Another paraphiliac offender, the ephibophile is exclusively aroused by pubescent children; however, even considered together, offenders with such insistently and involuntarily repetitive imagery or acts necessary for sexual excitement are a relatively small group.
Using “pedophilia” in a broader sense, Groth (1983) differentiated fixated from regressed pedophiles. The fixated individual is developmental^ arrested so that children remain his primary sexual objects and he fails to develop a sexual interest in adults. The regressed individual has had adult sexual relationships but reverts to an interest in children when frustrated in adult interactions. This theory does not address the concept of the paraphiliac offender per se.
Considering “pedophilia” in its broadest and most general sense as encompassing all sexual activity with or molestation of children, Araji and Finklehor (1985) reviewed the literature and attempted to summarize all the theoretical formulations within a four factor model: sexual arousal, emotional congruence, blockage, and disinhibition.
Sexual arousal. In order for an adult to be “turned on” by a child, there has to have been cultural or familial conditioning to sexual activity with children, victimization as a child, or early fantasy reinforced by masturbation.
Emotional congruence. For emotional congruence, there is a level of comfort and satisfaction in relating to a child and a fit of emotional need. Frequently, this is due to arrested development either through retardation, immaturity, or low self-esteem.
Blockage. Adult sexual opportunities may be blocked by traumatic experience with adult sexuality, sexual dysfunction, inadequate social skills, or marital disturbance.
Disinhibition. The pedophile may be disinhibited or lose control characterologically via impulse disorder, chronically via organicity or psychosis, acutely via alcohol, drugs, or situational stress, or culturofamilially via nonexistent family rules.
This broad definition of pedophilia would include the paraphiliac, fixated, and regressed pedophiles, and reflects the general population seen in clinical practice or the criminal justice system.
The four factor model is helpful not only in summarizing the literature and aiding in treatment formulation but also in understanding the characteristics of two subgroups of child molesters: the incest perpetrators and the female offenders.
Incest, by definition, occurs as part of a family system by blood relationship or household composition; however, the dynamics are explained by the four factors. Sexual arousal by children is not different from that experienced by other sex offenders but the family system may create its own blocking, disinhibiting, or emotionally congruent factors. If the spouse is physically and/or emotionally unavailable on a full or part-time basis, then a particular child or sequence of children may take on various maternal roles including that of sexual partner, often with the collusion of the mother. The child victim is often the “special” child who had been closest to the perpetrator. If the child already loves the perpetrator, it is relatively easy to misinterpret or exploit that love physically. The socially unskilled or “lazy” man need not look beyond his own home especially in the context of family and/or community acceptance of such behavior. A man may feel entitled to sex and dominant enough to demand that he not go beyond the family for gratification. Typically, those men who are aroused by the seduction process rather than the sex itself will not often find that challenge in the family setting. Study of children at risk suggests that the adult male’s lack of bonding to the young child because of absence through military service, work, travel, or incarceration might predispose that particular child to assault.
Failure to bond is also suggested as a major factor in the development of female pedophiles. Our work in progress has so far identified a small but consistent percentage of offenders as women. In addition to a sexually traumatic childhood, all have shown major disinhibition through mental retardation, psychosis, or severe character disorders. These dysfunctions not only interfered with maternal bonding but also contributed to suspended judgment about sexual contact with children, often in the company of a dominant adult male.
Abel, Becker, and Skinner (1985) have shown that once sexual contact is made with child, then others are at risk. Their sample of voluntary, nonincarcerated, anonymous offenders indicated that heterosexual pedophiles averaged 120 “attempted or completed child molestations.” Homosexual pedophiles averaged 205. Obviously, given this great number of victims for individuals who have not been arrested and the small number of victims for which even apprehended offenders are tried, there are many incidents unreported.
Pedophiles for whom that behavior is egodystonic or not seen as comfortable or appropriate may seek voluntary treatment; however, when sexual attraction to children is acceptable or egosyntonic, those individuals seek therapy only when threatened by the legal system or referred by it. For the therapist, there is often a conflict between abhorrence of the behavior, concern for the victim, and desire for punishment, and an understanding of the patient’s dynamics and desire to help him overcome his deviance. The ethical conflict is most intense when a patient reveals details about previously unreported victims and there is a legal obligation to report this behavior. Many therapists resolve this dilemma by taking referrals only from court or child-welfare agencies, instructing their patients about the limits of confidentiality, or limiting disclosure. It has been argued that this, in turn, is a disservice to untreated victims. There may be no good resolution to this dilemma.
As Araji and Finklehor (1985) summarized the literature about etiology, Kilmann, Satalis, Gearing, Bukstel, and Scovern (1982) summarized the literature about the treatment of pedophiles. There was no consistent approach and no theoretical basis for the treatment modalities which were utilized. Subsequently, Abel et al. (1985) outlined a multifactorial treatment approach which includes five treatment strategies: correcting cognitive distortions, providing sex education, promoting social skills, decreasing deviant arousal, and increasing nondeviant arousal. The first step in treatment is the development of an empathetic therapeutic relationship. Unless the patient perceives the therapist as an ally and is comfortable in expressing deviant desire, then it is impossible to make or monitor progress.
Correcting cognitive distortions. Cognitive distortions arise out of inappropriate attitudes and perceptions of sex roles and sex objects. Offenders may have difficulty in discriminating between sexual and nonsexual behavior or between coercive and noncoercive sexual behavior. These distortions must be corrected through education and insight-oriented therapy. First the perpetrator has to admit and accept responsibility for his own behavior. It is not generally true that sex-starved seven-year-olds jump out of the bushes and attack innocent, passing men. The “why me?” question can be addressed using the four-factor model and determining how the individual meets the criteria of each factor and how these combine to explain behavior. The role of the victim must be clarified as behavior may be rationalized by observations such as “she kept coming back” and the adult fails to take appropriate responsibility for his own actions. The effects on the victim should be considered as short-term responses of feeling used, different, afraid, guilty, isolated, embarrassed, or out of control and long-term responses of lack of trust, anger, low self-esteem, and confusion of intimacy and sexuality. Exposure to the effects of sexual abuse on the victim may lead into valuable work on the perpetrator’s own victimization.
A review of relevant state law and the legal process will reinforce the concept that adults are responsible. Statute defines the behaviors which society finds inappropriate. Individuals charged with violating these statutes must come to terms with the apparent arbitrariness of the judicial system. “It’s not fair” is the typical cry of the sex offender and he must ultimately come to terms with the reality of that observation. Seemingly irrelevant factors such as trial publicity, notoriety of the defendant, re-election promises, and concurrent cases may significantly affect the outcome of a case. In the early phases of therapy, especially pretrial, it is often impossible to deal with dynamic issues as the patient is so focused on the legal proceedings with inevitable delays, tactical positions, and the sense of victimization.
Providing sex education. Sex education may be necessary for those individuals who avoid or lack adult relationships because of fear and/or inadequate knowledge about sexuality. Treatment for specific sexual dysfunction may also be appropriate.
Promoting social skills. Training in social skills is also essential if the pedophile is expected to establish and maintain an adult relationship. Such skills include initiating conversation, maintaining a flow of t dk, learning about others’ interests, developing one’s own interests, sharing life stories, empathizing with others, asking for changes, and being assertive in meeting one’s own needs.
Decreasing deviant arousal. Several techniques have been developed to decrease deviant arousal; however, in order to insure effectiveness, one must be able to monitor that arousal pattern. Bradford (1985) has described penile tumescence examination using a strain gauge and polygraph recorder and charting erectile response to various visual or auditory stimuli. Such stimuli would ordinarily include color slides of various age groups of nude males and females as well as neutral controls, or audio tapes describing a series of sexual encounters. In some labs, the patient may make his own audio tapes. Bradford (1985) compares percentage of full erection to various stimuli to the average response to all stimuli. The patient must serve as his own control because of the wide variety of responses and degree of responsiveness in the population at large.
Many behavioral approaches have been effective in some cases in decreasing deviant arousal. The simplest may be thought stopping. When he experiences an undesirable thought, the patient thinks “stop” or some similar phrase to himself. If this is not sufficient, covert desensitization, also called cognitive aversive conditioning, may be tried. In this technique the patient pairs the thought of a negative consequence, real or imagined, with the undesirable thought. An example would be the experience of being kicked and tormented in a jail cell after arrest. The next level of behavioral treatment would be overt aversive techniques. Noxious olfactory stimuli such as valeric acid and ammonia are most common. Ammonia may be preferable because the patient may carry ampules and crush one under his nose when he experiences deviant thoughts. Electric shocks delivered in the lab have not been demonstrated to have long-term benefit. Ethical problems inherent in this treatment must always be considered. Any aversive technique may be undermined if the patient continues to masturbate to deviant fantasy outside therapy sessions.
Various medications have been used to decrease arousal. Thioridazine (Mellaril) and other major tranquilizers decrease arousal as a side-effect of treatment and have then been used primarily for this purpose. This is not a universal response and long-term use of the drugs may be risky. In Europe castration is utilized as punishment and to reduce the source of testosterone; however, only “chemical castration” is available in this country. Medroxyprogesterone acetate (DepoProvera) is an antiandrogen which lowers the serum testosterone level and reduces both sexual fantasy and the ability to perform. For those men who are overwhelmed by obsessive and intrusive sexual thoughts, it can provide great relief. Since that driven pattern of sexuality is not common, the drug is not commonly utilized. Berlin and Meinecke (1981) have described this treatment format including informed consent and monitoring of testosterone levels, weight, and blood pressure. DepoProvera injections are usually given weekly for a six-month period or may be continued longer with monitoring. Oral medication is not effective. Some controversy arises because the drug is presently approved only as an adjunct to the treatment of inoperable, recurrent, and metastatic endometrial or renal carcinoma and not for sexual appetite suppression. The ethical issue of the ability to give truly informed consent in a correctional setting or when threatened with same has also been raised. A similar drug, cyproterone acetate, is not presently available in the United States.
Abel et al. (1985) have described a very effective treatment known as masturbatory satiation. The patient quickly masturbates to orgasm and then continues to masturbate for one hour while making an audio tape of his deviant fantasies. This is monitored by the therapist for compliance. The deviant fantasies become boring and eventually aversive.
Increasing nondeviant arousal. The most common technique for increasing nondeviant arousal is that practiced during normal adolescence, masturbation to appropriate fantasy. Behavioral techniques such as systematic desensitization have also been utilized.
It has been argued that a group treatment approach is necessary for pedophiles. While this may be beneficial for those patients who require confrontation of their denial, recognition of their own and others’ irrational beliefs, and social skills training, there are those individuals who cannot or will not attend groups and the option of individual therapy should be available. The individual therapist must be able to offer the full range of dynamic, educational, and behavioral options, however. A therapist who is not comfortable with this population or these approaches should consider referral to someone who is. Names of experts are often available through departments of corrections, welfare agencies, medical schools, and professional societies.
An example of a comprehensive treatment program which is described in detail elsewhere (E. Rowen and J. Rowen, 1985; Rowan, in press) will be used to illustrate a sequence of therapeutic interventions. This inpatient program in a correctional setting is composed of three highly structured six month phases with a formal mechanism in place for promotion to the next phase.
Phase I. This introductory phase includes staff-led groups addressing social skills, sex education, legal education, and correction of cognitive distortion. Social skills groups emphasize modeling, role playing, and performance feedback. Assertiveness training and anger management are addressed in this phase. Cognitive distortions about sex roles and sex objects are challenged by peer group discussion of these false beliefs and interaction patterns. Each patient is asked to determine how he meets each of Araji and Finklehor’s (1985) criteria and to develop a group-approved treatment plan. A very powerful group exercise is a confrontation by women from an Adult Survivors of Incest group. This instills some sense of victim identification and sets the stage for future work on one’s own victimization. Patients also participate in a “self-help” group which they initiated. This Alcoholics Anonymous model group uses Carnes’ Out of the Shadows (1983) (formerly titled The Sexual Addiction) as its basic text. Patient leaders give tests on the content and this group also considers “relapse prevention” techniques such as recognizing the “MO” and then calling for help.
The group operates actively to both confront and support group members. For those patients who have difficulty in admitting responsibility to the group, the staff may go over police reports with them individually or later read them to the group if there has been no response to individual confrontation. Patients may also be confronted with the results of penile tumescence studies as entry level responses to standardized slides had been recorded.
Phase II. The intermediate phase is available to those who have demonstrated amenability to treatment by making satisfactory progress through Phase I. Therapeutic opportunities include social skills (stress management and communication skills in this phase) and individual therapy. A major focus of individual therapy is to target ways to decrease deviant sexual arousal. Each patient keeps a “fantasy diary” and is helped to develop meaningful covert sensitization responses as negative conditioners, or, if these are not successful, aversive techniques. Ammonia is the primary negative conditioner. Monitoring of penile tumescence to individual fantasy is done to measure the success of conditioned responses. DepoProvera is available for those who are unable to control fantasy in any other way; however, this obviously interferes with the objective monitoring of arousal patterns. Increasing nondeviant arousal is encouraged through masturbation to appropriate fantasy.
Phase III. Final phase patients may lead self-help groups and continue in individual treatment programs. Conjoint therapy is available if patient and partner wish. Social skills training includes life skills practice if near release into the community.
Self-report of progress is the most traditional but least reliable method of assessment. Prediction based on inclusion in a particular group or class is an alternative approach. Gross generalizations such as that homosexual pedophiles are more likely to reoffend than heterosexual pedophiles and that fixated pedophiles are more likely to reoffend than regressed pedophiles have face validity but may not be specific enough for individual prediction.
More objective standards may be based on the theoretical model with improvement demonstrated on each of Araji and Finklehor’s (1985) four parameters. For an individual patient, this may be that he is less sexually aroused by child stimuli based on penile tumescence monitoring or that he has agreed to continue DepoProvera with monitoring of testosterone levels. Blockage to meaningful adult relationships has been addressed through social skills training or therapy; the specific disinhibition has been addressed appropriately with approaches such as alcohol counseling, antipsychotic medication, or stress reduction; emotional congruence with children has been overcome with education and therapy.
Patients’ assessment of their own progress (or lack thereof) may be charted on rating scales and compared to therapist or staff assessment on those same scales. The greater the congruence among the patient rating, therapist rating, and other objective evidence of improvement, then the greater the confidence one may have in prediction.
The ultimate predictor might be the recidivism rate; however, given Abel’s (1985) data that a very small percentage of sexual assaults are reported, then rearrest would not be a reliable indicator of reoffense. Studies of the prediction of dangerousness and outcome of psychotherapy suggest that individual therapists feel quite confident in their personal predictions about their own patients; however, the overall predictions are no better than chance. There is no ethical way to monitor free individuals in the community. Monitoring of arrest records and probation reports is appropriate as long as the limitations are understood. We may be discouraged by our lack of objective evidence; however, our theoretical and subjective estimate of effectiveness may be the best measure we have and we must continue to treat this challenging population if we are ever to stop the cycle of child molestation—victim becomes perpetrator who creates further victims.
References
Abel, G., Becker, J., & Skinner, L. (1985). Behavioral approaches to treatment of the violent sex offender. In Roth L. (Ed.) Clinical Treatment of the Violent Person, pp. 100–123. Rockville, Maryland: National Institute of Mental Health.
American Psychiatric Association. (1980). Diagnostic and Statistical Manual of Mental Disorders, (3rd ed). Washington, D.C.: American Psychiatric Association.
Araji, S., & Finklehor, D. (1985). Explanation of pedophilia: Review of empirical research. Bulletin of the American Academy of Psychiatry and Law, 13, 17–37.
Berlin, F., & Meinecke, C. (1981). Treatment of sex offenders with antiandrogenic medication. American Journal of Psychiatry, 138, 601–607.
Bradford, J. (1985). The psychiatric evaluation of the sexual offender. Newsletter of the American Academy of Psychiatry and Law, 10, 18–19.
Carnes, P. (1983). Out of the Shadows. Minneapolis, Minnesota: CompCare, 1983.
Groth, P. (1983). Treatment of the sexual offender in a correctional institution. In Greer, J. & Stuart, I. (Eds.) The Sexual Aggressor, pp. 160–176. New York: Van Nostrand Reinhold.
Kilmann, P., Satalis, R., Gearing, M., Bukstel, L., & Scovern, A. (1982). The treatment of sexual paraphilias: A review of outcome research. Journal of Sex Research, 18, 193–252.
Rowan, E., & Rowan, J. (1985). Developing a treatment program for pedophiles. Corrections and Social Psychiatry, 31, 62–64.
Rowan, E. (in press). Predicting the effectiveness of treatment for pedophilia. Journal of Forensic Science.
Exhibitionism/Voyeurism{9}
Margretta Dwyer
Who exposes? Who voyeurs? What is the etiology of such behaviors? Can they be treated? These and many other questions haunt professional therapists. More sex offenses in general are being reported every day. Many of these people are mandated to a treatment program. If a therapist lacks experience in the treatment of sexual offenders it is frightening to assume this treatment. In a more serious vein, it is unethical to treat perpetrators unless the therapist has a solid program in place to do so. Treatment programs must have the capability of thoroughly assessing the exposer and voyeur, specifying their characteristics, and directing treatment goals towards the elimination or changing of these characteristics. This article will delineate in simple terms some treatment processes and refer the reader to research articles regarding others. Although only the issue of male sex offenders will be addressed it is fast becoming known that there are numerous female offenders “out there.”
Demographics of Sex Offenders
From an n = 200 at the University of Minnesota Sex Offender Treatment Program, 90% were white males, 58% had a current partner, 49% had some college or were college graduates, their mean age was 34.7 and their income was over $15,000 for 49% with 20% in the $20,000-$50,000 range (Amberson, Dwyer, & Tenley, 1986). Alcohol is a problem for only one-third of the offenders and this one-third are usually found to be incest perpetrators. In assessing exposers and voyeurs we have found no significant differences in their demographics as compared with other offenders except one —the exposer usually has a more extensive arrest record (Forgac & Michaels, 1982). An exposer will usually be arrested many times before he is considered serious enough for treatment. A voyeur’s arrest record is usually not as extensive as an exposer’s, but the voyeur is often taken more seriously sooner because of the proximity to personal property and being so close to victims’ windows, etc. Other sex offenses such as child molesting and rape are more immediately taken seriously on the first offense. Although our demographics are included here, these concur nationally with other programs’ demographics. Each reader will probably find similar demographics within his or her offender population.
Definitions
The word exhibitionism first appeared in the literature in 1877 (Myers & Berah, 1983) when Lasegue described this behavior as confined almost exclusively to males who apparently had sudden and over-powerful urges to genital display (Lasegue, 1877). He further states there is the absence of attempts to form a relationship with the victim and little effort to evade apprehension. Basically one hundred plus years later the description is no different. For a definition of voyeurism we rely on the DSM III (1980) which states that “Voyeurism is the repeated observation of unsuspecting persons who are naked, undressing, or engaged in sexual activity.” It is believed that almost all voyeurs are male. As with exposers, no attempt is made to form a relationship or engage in sexual activity with the victim (if sexual activity is sought or intended with the victim, the diagnosis should shift to a rape diagnosis). Further, voyeurs, too, are careless, making unnecessary noises, with little effort to avoid apprehension.
Etiology
Theories regarding the etiology of all sexual misconduct including exhibitionism and voyeurism are numerous. Diverse sources such as psychoanalytic theories, learning theories, and anthropol-
ogy, to name a few, offer possible reasons for the behavior but none have yet achieved experimental verification (Myers et al.) or medical verification. No single comprehensive theory explains paraphiliac behavior (Kilmann, Satalis, Gearing II, Bukstel, & Scovern, 1982). Some researchers attribute our identification with certain sexual arousals to our sex rehearsed play as children. Interference in this mapping (or love mapping) impairs the adult sexually (Money, 1984). This theory is based on evidence from sexual rehearsal play in childhood in the study of tribal peoples (Malinowski, 1929; Marshall & Suggs, 1971; Money & Ehrhardt, 1972; Money, 1980). Some believe, in conjunction with early interference, that there is a constant trying to “triumph over the trauma” (Stoller, 1975). That is, a critical happening occurs at a young age and the perpetrator is developmentally fixated at this age. “A certain event affecting sexuality” would be a good way to describe the interference Money alludes to or the “triumphing over trauma” that Stoller speaks of. Without clearly knowing the causes of exposing or voyeuring, researchers and treatment experts are able to agree on multiple characteristics of the sex offender as well as the numerous treatment components needed to offset these patterns/characteristics in the offender’s life.
An extensive battery of tests as well as numerous interviews are required to assess the advisability of treatment for an offender. Each program needs to develop its own assessment package. An example of an all-inclusive testing package is the one used at the University of Minnesota, Program in Human Sexuality, Department of Family Practice, Medical School. The following are included.
-
MMPI
-
Bern Sex Role Inventory
-
Derogotis Sexual Functioning Inventory
-
Tennessee Self-Concept Scale
-
Minnesota Sexual Behavior Survey
-
Locke-Wallace Marital Adjustment Scale
-
LoPicolo Sex Inventory
-
Multiphasic Sex Inventory
-
Milcom Health History Questionnaire
-
Psychophysiology Lab (Plethysmograph)
-
Physical Exam, including Testosterone and LH factor assessment
-
Assess for Depo-Provera
Besides the testing and laboratory workups, five to eight one-hour interviews are necessary, including interviews with the spouse. The spouse is also asked to complete appropriate testing. During this extensive assessment procedure no therapy should be included. This is difficult for inexperienced personnel as there is a tendency to shift from the assessment process to a therapy modality. Small segments of therapy may need to be interspersed with assessment when a man continues to have trauma around areas of job loss, court proceedings, separation from spouse, newspaper articles regarding him, etc., but most of this should be dealt with extensively after he is in treatment. There is a tendency for the offender to manipulate sympathy from the therapist and thereby keep the therapist from gathering all the history and data necessary for a good assessment.
Patterns and Characteristics of Offenders
In ten years of interviewing sex offenders at the University of Minnesota, we have observed and documented fourteen behavior and family relations patterns which we identify as characteristic of sex offenders. Although this comes from our data base, most of these patterns are found universally in sex offenders from other treatment programs. It is important to realize that these patterns must be looked at in “clusters” in the offender. Any normal person will have some or one or two of these characteristics. In a recent study on 56 new sex offenders coming into our program the following data was gathered:
TABLE 1 Tennessee Self-Concept Scale (n — 56)
| SCALE | % Under 20% | % Under 50% |
| Self-Criticism | 16 | 69 |
| Identity | 48 | 79 |
| Self-Satisfaction | 20 | 46 |
| Personal Adjustment | 27 | 54 |
| Social Adjustment | 29 | 59 |
-
A tremendous disdain for sex offenders exists among the offender population; therefore, the defense mechanism of denial must operate constantly in their systems so they do not label themselves as one of these “horrible” people. Ninety-three percent of our current population had this pattern. This was determined by the Tennessee Self-Concept Scale (Table 1), which measures self-esteem. Many were below the 50th percentile in areas of self-criticism (69%), Identity Scale or concept of “who I am” (79%), and Self-Satisfaction Scale (46%). This impression was also determined by the rater, by the offender’s use of self-deprecating words, and negative self-directed messages.
-
Offenders have a very poor or nonexistent relationship with their father, and often were ignored by their father throughout early development —thereby missing any nurturing touch from a male. This pattern is self-reported, but for better accuracy was also judged by the rater. Eighty-three percent of our offenders had this pattern. Judgment for this was based on consistently repeated statements such as “My father never noticed I existed” or “I never saw my father; he was always gone” or “My father never did anything with me.” Normally, reference to physical abuse was not included in their statements.
-
These are men who had overprotective mothers and/or later sought out overprotective wives who are primary enablers in their lives. Both the men and the women contribute to this unhealthy interaction. Offenders could not clearly self-report this situation since many were blind to it. Our rater found that 83% had this characteristic. Typically, mother or wife would respond during the intake sessions with protective statements regarding the offender. If a man was told what time his group would start, it was not uncommon to find the wife/mother writing down the schedule rather than the offender. Unable to sever bonds from his mother, a 30 or 40-year-old offender might still be living at home.
-
Offenders have often experienced an early sexual trauma, near ages 3–5, that contributes to their aberrant behavior. They develop their acting out behavior as a way to “triumph over this trauma” (Stoller et al.) and it becomes part of their adult sexual pattern. Forty percent of our population struggled with this characteristic as determined by the rater using case history. A man traumatized by severe beatings from his mother was still raping women and beating them; a man traumatized by having to continually attach his mother’s stockings and trying not to touch her legs was obsessed with making obscene phone calls to young girls, talking to them regarding their soft legs.
-
From a previous unpublished survey of 200 of our patients, 56% reported sexual or physical abusive experiences as children. With our present number of 56, we found only 36% remembering such incidences. However, many of these offenders are in beginning stages of treatment, and our experience has been that more patients will remember incidences as treatment progresses.
-
Obsessive religious codes are invoked by these men to justify repression of normal sexual activity, while they are, at the same time, violating socially acceptable norms. This religiosity is a less common pattern, but when it occurs, it is intense. Twenty-six percent were found by our rater and 7% by the Tennessee Self-Concept’s Moral-Ethical Scale to have this pattern. Although this religiosity seems paradoxical, it is an example of how they compartmentalize their sexuality. Statements such as “I was having sex with children because my religion forbids me to have premarital sex with adult women” or “I only had anal sex with my daughter because I wanted her to be a virgin” are common.
-
Most offenders are immature in either social skills, sexual skills, or both (Hall, Maiuro, Vitaliano, & Proctor, 1985). The Tennessee Self-Concept’s Social Scale indicated that 59% fell below the 50th percentile and the Derogotis Sexual Functioning Inventory (n = 46) placed 94% below the 50th percentile (Table 2).
-
Offenders generally exhibit low self-esteem and high self-criticism. The rater judged this pattern to be present in 98% of the sample. On the MMPI (n = 51), 33% of our sample scored below the t score of 50 on Social Introversion, and 31% scored below a score of 50 on Ego Strength (ES) (Welsh & Dahlstrom, 1956, Article 29).
-
Offenders see their sexual behavior as an outside force that “happens” to them. They do not take responsibility for this part of their personality. The rater judged 93% to have this characteristic. Such statements as “The child just happened to be in my bed” or “I had too much coffee that day” or “too much sugar that day,” gives an external locus of control to their sexuality.
-
In addition, many offenders feel a dissociation from self, as though someone else were acting, a quasi fugue state. The rater judged 84% of our sample to describe this quality about their offending behavior.
-
Offenders are generally passive. Their passivity further encourages the overprotective mother and/or wife to make decisions for them. Overall profiles from the MMPI, the Tennessee Self-Concept Scale, the Minnesota Sexual Experience Inventory, and the rater determined that 88% of the men had this pattern.
-
Associated with this passivity, offenders have tremendous amounts of repressed anger (Hall & Maiuro, 1986), yet, feel intimidated by other adults. Consequently, their behavior is often passive/ aggressive. The rater judged 76% to have this pattern.
-
Repression is a defense mechanism that is consistently used by the offender for his fantasy life and for sexuality. The patient thinks that repressing sexual thoughts will prevent his acting out. The repression scale (R) on the MMPI (Welsh & Dahlstrom, 1956, Article 26), the overall profile of the Derogatis (Table 3) and Minnesota Sexual Attitude Scales, as well as the rater, were used. Seventy-four percent were judged to have this pattern.
-
Manipulation is a key tool they have mastered in order to protect the dual lifestyle they must lead, i.e., being an upstanding businessman in the community, yet one who in his leisure time is sexual with children or exposing, etc. As determined by the rater, 93% had this pattern (Dwyer, Amberson, & Seabloom, unpublished).
Table 2: Derogotis Sexual Functioning Inventory (n — 46)
| SCALE | % Under 30% | % Under 50% |
| Drive | 30 | 48 |
| Experience | 46 | 61 |
| Attitudes | 74 | 83 |
| Affection | 72 | 83 |
| Overall Sexual Functioning | ||
| Inventory | 76 | 94 |
Seventy percent of a sample had 11 of the patterns. Eighty-three percent had 8 patterns. It is believed important when looking for an offender’s profile that only clusters of these patterns be admitted as evidence of a profile so as to distinguish them from normals who may have only a few of the patterns.
Table 3: MMPI Scales and Scores (n — 51)
| Scale | t scores | |
| Below 50% | Above 50% | |
| K Scale{10} | 94% | |
| Scale 4 | 88% | |
| Scale 6 | 86% | |
| Scale 8 | 78% | |
| R Scale | 65% | |
| ES Scale | 31% | |
| CN Scale | 39% |
These patterns described have received support in the literature. The mechanisms of repression and denial have long been observed to have a connection to offending behavior (Dwyer & Amberson, 1985), as have early childhood experiences and family of origin issues (Money, 1970). The lack of social and sexual skills has been documented, as well as the need for sexual information (Schwartz & Masters, 1983; Abel, Blanchard, & Becker, 1977; Eisler, Miller, & Hersen, 1973).
One consistent result from studies in the past shows the lack of psychopathology found in exhibitionists (Langevin et al., 1978; McCreary, 1975; Rader, 1977; Smukler & Schiebel, 1975). Although similar studies are not available for voyeurs, clinical observation and testing indicates a lack of psychopathology.
Exhibitionists tend to be younger than voyeurs or pedophiles. The peak of exhibitionism is in the twenties and decreases over the thirties, with symptoms occurring only rarely in the forties (Mohr et al., 1964). Although this study is old, clinical observation would indicate it is fairly accurate for 1987.
Therapeutic Interventions
Because sex offending behavior has multiple dimensions, an intensive therapy plan must be operational in order to help the offender. Most sex offender therapists have learned through the years that separating different kinds of sex offenders (voyeurs, exposers, pedophiles, etc.) for treatment is not necessary or helpful. Offenders’ traits are very similar; therefore treatment components can be almost identical with a few individuated variations for each family and offender. For example, sometimes a separate group for their spouse may be required, and sometimes it may be optional. Some men will receive different behavioral assignments, different reading assignments, etc.
Covering treatment components is too lengthy to be done in a short paper. However, some of the University of Minnesota’s plan can be briefly presented. The University’s care is based on countering the fourteen patterns found in the offender. Sixteen goals were
developed in order to accomplish this. The sixteen goals are as follows:
-
Stop the offending behavior and be able to define “at risk” situations.
-
Be able to admit to and take responsibility for their role in the inappropriate and appropriate sexual behaviors.
-
Arrange for and attend appointments for all parts of the treatment; i.e., family therapy, therapy with P. 0., group, SAR, spouse’s group, etc.
-
Participate in the group to the extent that (s)he shares thoughts, feelings and new learning with the group and responds to other group members’ comments and feelings openly.
-
Learn new problem-solving strategies which are not self-defeating, and be able to appropriately apply these strategies.
-
Thoroughly examine any sexual behavior that has caused problems, identify the origins and meanings of the problem, and share this insight with the group and family.
-
Develop a plan to prevent further offending behavior by:
-
identifying the patterns which contribute to the offending behavior
-
changing the patterns
-
implementing a program to maintain these changes.
-
Experience empathy and understand how sexual behaviors affect others.
-
Define his/her family role.
-
Improve communication with their family by sharing feelings, discussing conflicts, improving listening skills, and understanding the origins of conflict.
-
Acknowledge and accept their fantasies without fear, be able to describe fantasies, to increase enjoyable fantasies, and to learn that fantasy does not cause behavior, but that behavior is based on choice.
-
Demonstrate an understanding of body messages and be able to share the meaning of these with others.
-
Define his/her sexual needs and be comfortable expressing these needs appropriately.
-
Move from passive, helpless, and dependent behavior to more assertiveness in his/her relationships.
-
Demonstrate a more positive attitude and an ability to enjoy all areas of life-work, friendships, family relationships, and leisure activities.
-
Understand and integrate his/her sexuality into his/her intellectual, social, and spiritual self.
In order to accomplish these goals, numerous therapy modalities are used, including psychoanalytic theory, structural and strategic family therapy, social skills modalities, behavioral techniques, and cognitive restructuring, to name but a few. Always an eclectic approach is maintained. Recidivism is almost null (Dwyer & Amberson, 1985) when an excellent program is in place.
References
Abel, G. G., Blanchard, E. B., & Becker, J. V. (1977). An integrated treatment program for rapists. In R. Rada (Ed.), Clinical Aspects of the Rapist (pp. 161–213). Orlando, Florida: Gruñe & Stratton.
Amberson, I. J., Dwyer, S. M., & Tenley, J. (1986). Bern Test Comparisons: Normals with Sex Offenders. Unpublished paper presented at NIMH meeting, Tampa, FL.
Dwyer, S. M., & Amberson, I. J. (1985). Sex offender treatment program: A follow-up study. American Journal of Social Psychiatry, 4.
Dwyer, S. M., Amberson, I. J., & Seabloom, W. (1987). Personal and familial characteristics in sex offenders. Unpublished manuscript.
Eisler, R. M., Miller, P. M., & Hersen, M. (1973). Components of assertive behavior. Journal of Clinical Psychology, 29.
Hall, G. N., & Maiuro, R. D. (1986). The assessment and treatment of anger problems in sexually assaulted males. Paper presented at NIMH conference on Assessment and Treatment of Sex Offenders. Tampa, FL.
Hall, G. N., Maiuro, R. D., Vitaliano, & Proctor, W. (In press). The utility of the MMPI with men who have sexually assaulted children. Journal of Consulting and Clinical Psychology.
Kilmann, P. R., Satalis, R. F., Gearing, M. L. II, Bukstel, L. H., & Scovern, A. W. (1982). The treatment of sexual paraphilias: A review of the outcome research. Journal of Sex Research, 18, 193–252.
Langevin, R., Partich, D., Freeman, R., Mann, K., & Handy, L. (1978). Personality characteristics and sexual anomalies in males. Canadian Journal of Behavioral Science, 10, 222–238.
Lasegue, C. (1877). Lex exhibitionists. L’Union Medicate, 23, 709–714.
Malinowski, B. (1929). The Sexual Life of Savages in Northwestern Melanesia. New York: Halcyon House.
Marshall, D. S., & Suggs, R. C. (Eds.). (1971). Human Sexual Behavior: Variations in the Ethnographic Spectrum. New York: Basic Books.
McCreary, C. P. (1975). Personality profiles of persons convicted of indecent exposure. Journal of Clinical Psychology, 31, 260–262.
Mohr, J. W., Turner, R. E., & Jerry, M. B. (1964). Pedophilia and Exhibitionism. Toronto: University of Toronto Press.
Money, J. (1984). Paraphilias: Phenomenology and classification. American Journal of Psychotherapy, 38(2), 164–178.
Money, J. (1980). Love and Love Sickness: The Science of Sex, Gender Differences, and Pairbonding. Baltimore: Johns Hopkins Press.
Money, J. (1970). Paraphilias: Phyletic origins. Unpublished manuscript, Johns Hopkins University.
Money, J., & Ehrhardt, A. A. (1972). Man and Woman, Boy and Girl: The Differentiation and Dimorphism of Gender Identity from Conception to Maturity. Baltimore: Johns Hopkins Press.
Myers, R. G., & Berah, E. F. (1983). Some features of Australian exhibitionists compared with pedophiles. Archives of Sexual Behavior, 12, 541–547.
Rader, C. M. (1977). MMPI profiles of exposers, rapists, and assaulters in a court services population. Journal of Consulting and Clinical Psychology, 45, 61–69.
Schwartz, J. F., & Masters, W. H. (1983, Spring). Conceptual factors in the treatment of paraphilias: A preliminary report. Journal of Sex and Marital Therapy, 3–18.
Smukler, A. J., & Schiebel, D. (1975). Personality characteristics of exhibitionists. Disorders of the Nervous System, 36, 600–63.
Stoller, R. J. (1975). Perversion: The erotic form of hatred. New York: Pantheon Books.
Welsh, G. S., & Dahlstrom, W. G. (Eds.) (1956). Basic readings on the MMPI. Articles 26 and 29. In Psychology and Medicine. Minneapolis: University of Minnesota Press.
Obscene Phone Callers{11}
Ord Matek
The Diagnostic and Statistical Manual of Mental Disorders-DSM III (1980) makes no specific mention of the Obscene Telephone Caller, other than to note “Telephone Scatologia (lewdness)” under the classification 302.90 Atypical Paraphilia, “deviation (para) is in that to which the individual is attracted (philia)” (p. 275). Despite the fact that it is listed alongside quite bizarre paraphilias, the behavior of the obscene telephone caller is of a different magnitude than most of the paraphilias named with it: Coprophilia (feces); Klismaphilia (enema); Mysophilia (filth); Necrophilia (corpse); and Urophilia (urine). It is listed in this category because it meets the criteria for a paraphilia and because it cannot be classified in any of the other categories.
The essential feature ... (of a paraphilia)... is that unusual or bizarre imagery or acts are necessary for sexual excitement. Such imagery or acts tend to be insistently and involuntarily repetitive and generally involve either: (1) preference for use of a nonhuman object for sexual arousal, (2) repetitive sexual activity with humans involving real or simulated suffering or humiliation, or (3) repetitive sexual activities with nonconsenting partners, (p. 266)
The DSM III further instructs us that “individuals with these disorders tend not to regard themselves as ill, and usually come to the attention of mental health professionals only when their behavior has brought them into conflict with society” (p. 267). Unfortunately, no additional information is forthcoming from DSM III on the Atypical Paraphilias which are a residual category. This is in contrast to the specific paraphilias that are more Zoophilia, Pedophilia, Exhibitionism, Voyeurism, Sexual Masochism, and Sexual Sadism. With each of these, a brief informative description is provided which not only details the behavior but lists whatever may be known as to prevalence, predisposing factors, age at onset, and course of the disorder over time. Specific diagnostic criteria are also given. Certainly a lot more information than the three words given to the Obscene Phone Caller, “Telephone Scatalogia (lewdness).”
The sparcity of DSM III information should not lead one to the conclusion that the phenomenon of the obscene telephone call is surprisingly high. Almost one of five complaints directed to the New York City telephone company reported obscene calls (Nadler, 1968). The approximate number of obscene phone call complaints directed to the phone company in that city in that year alone was more than 17,500. In addition, it is likely there were obscene calls that were never brought to the attention of the authorities. In a survey of college female undergraduates, Murray concluded that nearly half the females who responded had received such calls (1967). In a follow-up study the number was even higher. Murray and Beran (1968) reported that 75 percent of the female undergraduates who were surveyed had received obscene phone calls. Moreover, with the development and proliferation of crisis telephone centers, a new phenomenon is now being seen. Brockopp and Lester (1969) have written that a number of males telephone these “hot lines” for the sole purpose of masturbating while talking to a female counselor. It is likely that there is not a single crisis telephone program anywhere in the U.S.A. that has been free of these telephone masturbators.
There are no current studies that might update the information as to the prevalence of obscene phone calls, but one can expect the incidence of such calls is at least as large as previously determined if not greater. The last published data (Adams and Chiodo, 1983) reports that obscene phone calls are so frequent that virtually all women and quite a few men have received such calls.
General consensus identifies the obscene phone caller as male. Contributing to the general consensus that identifies the obscene phone caller as male is the data established by various investigators that show sexual deviations to be much more pronounced in males than females. This is not to say that there are no known instances of females engaging in the same behavior. However, they are seen as far fewer in number—to the point of rarity, and, in addition, are understood as having altogether different dynamics motivating their behavior.
Russell (1976) writes from his experience in criminal court clinics:
Harassing, threatening, vituperative calls by women, often replete with obscenities are not uncommon. However, these are most usually an expression of intense rage at some real or fancied rejection and are directed at an involved party... Some of these women are quite emotionally disturbed, some paranoid, and obscene telephone calls are sometimes perpetuated (sic) by women suffering from manic-depressive psychosis, (p. 11)
Perhaps the epidemiological information may be incorrect, and there are indeed more female obscene phone callers than is generally believed. Even were the underlying dynamics of such female callers the same as those of the male obscene telephone callers, the phenomenon is not the same. Male recipients of such calls are not likely to feel frightened and violated by a female obscene phone caller, in the same way as does a female recipient of the anonymous male caller; the intrusive call is more likely to be shrugged off by a male “victim” if not actually enjoyed as a kind of titillation. It is not likely to be reported to the authorities, nor seen as an ominous event. We are all (male and female) products of a society with a double standard with regards to many aspects of sexuality. (A male observing a female at her window while she is undressed may be charged with being a voyeur. A male observed by a female at his window while he is undressed may be charged with being an exhibitionist.) In any event, obscene phone calls from women are rarely reported to the authorities.
The behavior patterns of obscene telephone callers vary greatly. Generally, they do not select a specific victim, but choose numbers at random from the phone book, or by chance dialing. Sometimes they masturbate during the telephone encounter. Others stimulated by the telephone experience may masturbate afterwards (Russell, 1971; Gebhard, R. H., Gagnon, J. H., Pomeroy, W. B. and Christenson, C. V., 1965). On occasion an individual will memorize a telephone number and name of a female while standing in line behind her as she pays her bill by check in a supermarket or some other business with checkout lines. He will then call anonymously and terrify her all the more in that he knows her name, address, general physical appearance, some food preferences, etc. (author’s case files). Some obscene phone callers do not speak. Instead, they emit sounds of sexual pleasure into the phone, or breathe heavily. Others reveal their masturbatory activity to the victim. Sometimes it is clear to the victim that the man on the phone may be intoxicated because of slurred speech, mild incoherence, etc. Other callers are simply crude and utter profanities and obscenities. Some callers bluntly ask for sex and otherwise make inappropriate overtures for getting together. More sophisticated callers profess to know the victim through a mutual acquaintance or by having met at a social gathering. There are also obscene phone callers who present themselves as “taking a survey” with the respondent’s data to be kept confidential as they ask increasingly personal and private information. Alternatively the caller may present himself as a policeman or representative of a manufacturer of feminine products (vaginal douche, menstrual pads, etc.) with a “recall of product” warning and discussion of symptoms. Sometimes instructions will be given: “Open your legs and look to see....”
Mead (1975) chooses to classify the types of obscene phone callers into three major groupings. In the first group, which he calls the most common, is the caller who proceeds almost immediately to use profanity and/or make obscene propositions. The majority of these callers Mead believes are juveniles. Mead calls the second group “the ingratiating seducers.” In this instance the caller intrigues the woman with a somewhat believable story of mutual friends or previous contacts or his admiring of her from afar, until ultimately, he manages to raise her suspicions or he finally offends her. This caller, Mead cautions, may become a repeat caller particularly if he gets the victim to talk even briefly on subsequent calls. The third group is named the “trickster.” This refers to individuals who falsely present themselves or someone with a “legitimate” reason for talking with the victim about personal matters (survey taker, etc.).
The telephone masturbators who call a crisis telephone center are not easily fitted into Mead’s three major groupings except in rare instances. The female crisis line volunteer may be asked a legitimate question by the caller. In fact, it is often the kind of question commonly asked by many callers — except that this caller is interested in the woman’s voice and her response to him, more than the “answers” she may provide. The caller may profess problems of impotence with a request for guidance. Or he may inquire as to how does one go about pleasing a woman, or ask for information as to how can a man tell if a woman is “turned on.” All the while he is likely to be masturbating. If the woman does not realize this from the tones of his voice and/or his breathing, he is likely to inform her. If she turns the call over to a male volunteer, he hangs up. If she hangs up on the caller, he is as likely as not to call back or call another crisis phone service if one is available (author’s case files). Moreover, these callers generally are repeat callers. The volunteers over time get to recognize their voices, their style of talk, etc. and even assign identifying names for them in their conversations with one another at their regional crisis line conferences. This is not to say that they are unperturbed by being exploitively used as an unwilling sex object. It bothers them greatly (author’s case files).
Explicit sex conversations with unwilling listeners are illegal. But even with modem technology it is not always simple to locate the perpetrator of such calls. The information, therefore, that accurately describes the personality makeup and the underlying dynamics of the obscene phone caller is insufficient. It is based on too small a sample — those who were somehow apprehended or discovered and available personal history for study. Gebhard et al., in a sample of 1356 males convicted as sexual offenders, found only 6 obscene telephone callers (Gebhard et al., 1965). Of these six, three were also exhibitionists. What has been written suggests a similarity to male exhibitionists (Gebhart et al., 1965; Nadler, 1968). In fact, Lester (1977), in discussing telephone counseling and the masturbator, particularly makes reference to psychotherapy with exhibitionists by way of emphasizing some of the obstacles in therapy by telephone with the masturbator who exploits the crisis telephone services.
It is not difficult to find parallels in the behaviors of male exhibitionists and male obscene telephone callers. Sadoff (1976), in his discussion of sexual deviations, separates what he describes as “aggressive” deviations (such as rape, pedophilia, sadomasochism) from a second group which he calls “anonymous” deviations. He defines this latter group as sex behaviors “that appear to be on a continuum and yet involve gradually decreasing contact with the object of sexual desire” (pp. 430–431). He lists frottage (anonymous furtive sexual contact with a selected victim in a crowd) at one end of his continuum and moves through exhibitionism, voyeurism, obscene telephone calling, and finally, fetishism at the other end of the continuum. The anonymity he suggests is important in that it defends the perpetrator from the anxiety he experiences with respect to “direct confrontation or contact with the desired sexual object” (p. 432). It is Sadoff’s belief that these “anonymous” sex deviates may fantasize having sexual intercourse but are too anxious about it to be able to really go through the process of doing so.
The best brief statement that may help clarify the behavior of the exhibitionist (and, to the extent of similarity, the obscene phone caller) can be found in Hobson’s (1983) explanation of exhibitionist motives. He writes, it is
... a complex and multidetermined behavior that may serve a variety of purposes for different individuals. For some, it is a way of expressing aggression and hostility in a manner that usually does not result in counter-aggression. For others, it is a means of demonstrating their power over others (especially when the victim reacts by losing her self-control ....). In some cases, exhibiting is an attempt at asserting their masculinity and gaining recognition or approval, and finally, for some men the behavior is a way of validating themselves to compensate for their sense of inadequacy, (pp. 91–92)
Hobson further states “like any symptom it in part expresses a need, reflects a conflict and defends against anxiety. It never resolves the underlying problem and therefore becomes self perpetuating and self defeating” (1983, p. 92).
Perhaps the most important characteristics of the obscene phone caller are poor self-esteem and probably anger toward women (derived, says Nadler, from the relationships with mother; Nadler further describes their mothers as dominating, overprotective, and bossy) (Nadler, 1968; Mead, 1975). Despite the persistent symptomatology, the obscene phone caller is generally not viewed as dangerous (Mead, 1975; Russell, 1971; Sadoff, 1976).
While it is certainly useful to project the psychodynamics of the exhibitionist onto the obscene phone caller, some additional information seems warranted. These are not always distinct and mutually exclusive groups. Some obscene phone callers are also exhibitionists (Nadler, 1968). But this is not always the case. Those who are exclusively obscene phone callers provide themselves with greater anonymity than the exhibitionist (Sadoff, 1976). Does this imply that their anxiety level about actual sexual contact is greater? Or, perhaps, it is their fear of apprehension that is greater? Given Hobson’s excellent description, one looks also to his other listed objectives for differences in magnitude that might better differentiate the personalities that comprise these two groups: difference in intensity of aggression/hostility to women; greater fear of retaliation; etc. We do not know.
That the telephone deviant hears but cannot actually see the victim (whereas the exhibitionist both sees and hears her) suggests that his use of imagery plays an important part in his mode of building sexual excitement. He undoubtedly supplements the auditory clues with his own visualizations of what may be happening at the other end of the telephone connection. He can “see” her and chooses to believe she cannot “see” him. His control in the situation, in part, consists of his imposing himself while not exposing himself. Both exhibitionist and obscene phone caller require that a woman respond with some degree of shock, disgust, or upset (Hobson, 1983; Mead, 1975). This kind of reaction feeds into their sense of power/ control and establishes that their objectives have been met. But the imagery skills of the telephone deviant serve well enough for this purpose. The actual physical presence of a female is not needed and may even interfere with his game plan. He is free to masturbate at that time (if that is his modus vivendi), and/or recall the experience in later sexual fantasy with no concerns about setting up the experience and escaping it afterwards, to intrude on the event. Even if the phone event fails, there is immediate access to a replacement female just by dialing another number. Sexual energy is not lost in the process of search for victim. The physical appearance of the victim is irrelevant. Her age, appearance, etc. are not able to deter the caller. He makes her in the image that he chooses.
There is yet another aspect in phone contacts that is noteworthy. The telephone connection provides a pseudo-intimacy. The voice of the other is immediate. It allows both intimacy avoidance along with a sense of proximity. The obscene phone caller gets both: anonymity and closeness.
This paradoxical combination of anonymity and proximity is a most powerful inducement. One sees its force when one is confronted with the information that reveals the magnitude of “legal” telephone sex. Today, nearly every pornographic magazine carries advertisements giving telephone numbers one can call for a sexually explicit conversation. Most of these advertisements carry photographs showing or suggesting nude/near nude women in lewd contexts. For a fee chargeable to a credit card, a man can call any of these numbers and a woman will “talk dirty” with him, for him, or even at him. This commercial utilization of anonymous phone sex is a large and lucrative operation. Time magazine reported (1983) that one such New York City number attracts 500,000 calls daily which earns $25,000 per day for the phone company. The business owners of course do even better. Insofar as these calls do not involve an absence of consent for either of the persons engaged in the lewd conversation, they have so far not been declared illegal.
Not altogether surprising, therefore, is that computers with the same possibility of anonymity and proximity can stir up issues of pseudo-intimacy and sexuality. At $6 to $8 per hour people can sign on certain channels for open conversation via their personal computers with any and all who may be available at that moment. Obscene content is not always a part of this chatter but the names of “handles” chosen by many of these participants divulge a sexual implication: Honey Blonde, Priapus Rex, Wet End, Love for Tender, Bilady Jugs. At times the “conversation” too is suggestive and occasionally the computer screens read like a pornographic novel, as two or more strangers engage in “computer sex” with each of the participants describing successive steps in their fantasy encounter (Wrenn, 1985).
It is of interest to this writer that the literature on the psychodynamics, objectives, and behavior of the obscene phone caller does not speak to the aspect of the fantasy/imagery ability of the perpetrator. It would seem to be a necessary tool for him in his attempts to manipulate his victim, and to derive his own erotic gratification from the process. Indeed imagery/fantasy is an important component of all sexuality. The noted sex therapist, Helen Singer Kaplan, says “good sex is a mixture of friction and fantasy” (Kaplan, 1974).
Sexual fantasies are mental images of erotic experiences. They can occur during actual sexual activities (autoerotic or partner related) or isolated from actual sexual experiences. Schwartz and Masters (1984) calculated a modal average of eight fantasies a day in their interview sample of 120 men and women.
Freud (1953) thought that fantasies acquired a sexual excitement by being connected over time with sexual experience (i.e., masturbation). He wrote,
The masturbatory act consists of two parts, one of which was the creation of the fantasy and the other a manipulative performance for attaining auto-erotic gratification at the climax of the fantasy. It is known that these two components of the act have first had to be welded together. Originally, the active performance was purely auto-erotic, proceeding for the purpose of attaining pleasure from a particular erotogenic part of the body. Later, this performance became bound up with the idea of a wish emanating from the sphere of object-love and as a particular realization of the situation in which the fantasy culminated, (p. 51)
Sexual fantasies including fantasies involving deviant sexual behaviors were viewed by Freud as emanating from instinctual sexual drives. Freud initially described perversions as the expression of infantile sexual cravings. In normal development these are converted into heterosexual activity or into neurotic symptoms as a defense against their expression. However, where there might be a failure of these defenses, the perversions would result (Freud, 1953).
McGuire, Carlisle, and Young (1965) approach the issue from a learning theory perspective rather than a psychoanalytic one. Their belief is that sexual variations are learned. Any stimulus preceding ejaculation in a critical time interval becomes more sexually exciting. This can happen accidentally or deliberately. That is to say the stimulus may be introduced by plan (as with pornography or deliberate fantasy) or the stimulus may spontaneously/accidentally occur. Their belief is that sexual learning occurs after an initial early sexual experience of whatever kind, and later experiences modify the learning in a variety of ways. Sexual fantasy they believe is built on these learned variations. Like Freud, they give an important position to masturbation in the sexual learning process. The early sexual experiences play a role in providing the scenarios for later masturbation. To the degree that these theories are valid, the masturbating obscene telephone caller may be continually reinforcing his pattern.
As regards the simultaneous wish for both closeness and distance the literature on psychoanalysis and on object relations theory includes volumes on the need-fear dilemma. Seeman (1974) (in explaining the obscene speech of psychotics) gives us inadvertently another glimpse into the dynamics of the obscene telephone caller. She writes “(It allows)... a tremendous need for closeness and an equally strong fear of intimate human contact. Bringing sex into a casual conversation illustrates the dilemma and provides its own solution” (p. 199).
Seeman is writing about what she believes is the core problem of schizophrenia. But the need-fear dilemma may explain specific behaviors in non-schizophrenics when that behavior is a defense against perceived external or internal ego threats. The obscene phone call indeed is just that —in a multifaceted way. It allows safe expression of aggression/hostility at women in general in a doubly safe way. The mother is preserved as a love object because the anger is discharged elsewhere. Moreover, the hostile/aggressive expression is safe because retaliation is unlikely. There is proximity enough to strike out, but distance aplenty in which to be safe. Furthermore, the process provides a feeling of superiority in that the victim is perceived as inferior in her helplessness and impotent outrage (as the obscene phone caller probably was many times in his own growing up). Also, there is a sense of superiority in the getting away with flouting social norms.
These are not men who are unable to engage in actual sexual intercourse (Sadoff s contrary statements notwithstanding). Nor are they incapable of meaningful relationships with women as the following case histories demonstrate. In fact, the deviant sexual expression may preserve the significant intimate relationships they do make as the behavior allows the disturbing feelings to be bound up and directed elsewhere.
Ken, referred for counseling at age 23, began making obscene phone calls at the age of 14. Despite discovery on at least two occasions, followed by personal discussions about this with his minister, he continued in the activity. He feels the urge “to make a call” when he is alone for a long time and “gets to thinking.” (Author’s comment: when his introspection moves him to confront depressive feelings.) His parents are divorced and were separated when he was eight. He lived with both his mother and father, unhappily in both instances. His father’s second wife resented him, as an intrusion in their life, and his mother is critical and demanding of him. He has a girlfriend who is outgoing and attractive and quite jealous of the many women who express interest in Ken at his work as a bartender trainee. He is tall, with a muscular build, and rugged good looks and has a somewhat shy interpersonal style. His girlfriend is aware of his problem behavior and is puzzled deeply by it. Ken cannot explain it to her, nor to himself. In therapy he concedes that it expresses elements of anger and getting even. When he first began, he would even repeat to himself “I’ll show them” before he made his calls. On rare occasions, he has masturbated in front of the TV when the program featured closeups of women. He pretends they can see him and cannot do anything about it. He has not engaged in any other exhibitionistic behaviors. The sexual relationship between Ken and his girlfriend seems satisfactory to both. In fact they are discussing marriage (author’s case files).
Mr. L., married six years, is a successful advertising writer. He is both an exhibitionist and an obscene telephone caller. He is in therapy as an alternative to jail as he had been recently arrested for the third time for exhibitionism. His wife is a court reporter and they met in the course of her work at one of his trials. She is an extremely attractive woman who says he is the most handsome man she has met. He is indeed handsome and well-dressed. They report no particular discord in their childless marriage although there are occasional small disagreements.
Mr. L. describes the problematic sexual pattern as beginning in high school. He was a social outcast and felt especially scorned by some of the more popular girls who seemed to go out of their way to publicly taunt him. He felt that his strict religious upbringing and out of date hand-me-down clothes set him apart. He also could hardly see without his thick glasses and these girls would sometimes snatch them from him and humiliate him about his blind, unkempt appearance (he now wears contact lenses and spends a lot of time and money on his wardrobe). Home was not a refuge for him. His father was remote and his mother vacillated between ignoring him and criticizing him. She had wanted a girl and when their only child turned out to be male she was disappointed and never let him forget it.
Mr. L. would find his victims by driving around to locate the right circumstances and person. Then he would briefly exit his car, get her attention, while executing masturbatory motions on his exposed penis, then retreat to his car, where he quickly drove around the nearest corner. Later he would masturbate to orgasm with recall of the incident, especially the horror on the woman’s face, to fuel his excitement. His obscene telephone calls are more frequent at night rather than day. They are likely to occur when he has been working hard in the office after others have left. He describes a particular kind of excitement that he feels in this familiar place that is now deserted and darkened. He usually leaves the office to call any random number until a female voice answers. He masturbates later back at the office (author’s case files).
In addition to encapsulating together the troublesome feelings and the deviant behavioral discharge, the obscene phone call provides excitement. This it does on two levels. There is not only the excitement that is found when engaging in forbidden activity, but also the sexualized aspects of the encounter provide erotic excitement to the caller albeit at the expense of the victim. The feelings of control and power additionally convey feelings of greater pseudo virility to the caller. This serves as an ego restorative to the caller’s feelings of low self-esteem. He is also validated in his masculinity in his use of his sexual maleness in the perverted conquest of the female victim. Her horror, disgust, and upset convey this validation to him along with the sexual titillation he gets from it. The caller does not have to negotiate a relationship. He imposes it with no concession to the other. The phone conversation is on his terms. Not only is the risk of discovery and apprehension minimal, but the risk of failure is also low. A dissatisfying phone call can immediately be remediated by calling another number. No wonder the deviant behavior is pervasively engaged in by the obscene phone caller.
It would not be fair to discuss the obscene phone caller without some suggestions to guide the women who might be plagued. The best thing to do is to hang up the phone gently with the realization that this is an obscene phone caller. Banging the receiver down or trying to retaliate by screaming or scolding only plays into the wishes of the obscene phone caller who takes this as reward. Some women have reported success by partially covering the mouthpiece of the phone and saying out loud, as though talking to a third party, “This is him, officer —hurry.” Other tactics that seem to have worked are to pretend to be hard of hearing and to complain that it is difficult to understand him; or to say one is going to another phone extension, but instead, just let the phone sit off the hook for a while. The phone company says these are not necessary. Hanging up gently is enough. If the phone rings again immediately afterwards one should not answer it. It is not wise to blow a loud whistle into the phone as the caller may call back and do the same to the woman. The phone company will help when the calls continue over time. They should be notified.
The recommendation to those who serve as volunteers at a crisis phone service is very different. Here there is a dilemma as Lester (1977) aptly points out. The crisis phone service is set up to help troubled people and the volunteer has been trained to do this. But to engage with the telephone masturbator, who certainly needs help for his deviancy, is to become involved in his sexual scenario. Matek (1980) recommends a brief response that reflects the caller’s problem and suggests therapy, “it’s so sad that you are confusing sex by yourself with your inability to feel right unless you are intimidating a woman. Please get professional help.”
Therapy with obscene phone callers should be based on the type of caller and also should take into account whether the caller is mandated into therapy or self-motivated.
In the instance of juveniles, where there is a history that evidences faulty self-esteem the phone calling is a more serious situation than when it is not symptomatic but represents primarily adolescent experimentation. In the former instance, family therapy may be useful and unnecessary in the latter.
Early adolescent experimentation may sometimes take the form of making obscene phone calls. It is a stage in life where sexual drive and interest for boys may be quite advanced and at the same time beyond their social development. There is a tremendous wish for some kind of “sexual contact” and poorly developed or lack of social skills that may allow for participating in an intimate male-female relationship. An anonymous sexually oriented phone call (sometimes to a specific female) is a temporary “solution.” It does not necessarily augur pathological process, nor future obscene phone use. Pathological process or not, it is still a frightening and unwanted intrusion for the female victim. While the act is deviant, it warrants a different intervention than is needed for the habitual adult obscene phone caller. Time with maturation will likely lead to better adaptation and a cessation of the intrusive calls. Facilitating social contact (as for example via boy-girl group discussions and informal activities) may be enough for some —along with individual sessions with the youngster to identify the concerns and normalize the behaviors.
Of much greater concern are those instances in adults as well as juveniles where serious mental and/or severe physical problems are the cause for a pattern of making the intrusive sexually oriented phone calls to women. The distortions of psychotic process often present with an emphasis on sexual expressiveness and typically inappropriate sexual expressiveness. Seeman (1974) suggests there are psychodynamic motivations to help us understand the bewildering phenomenon of psychotic sexually exaggerated speech. Regardless of our understanding, it is clear that the sexually offensive behavior of psychotics cannot be successfully addressed, except as the basic pathological condition of psychosis may be ameliorated.
An equivalent problem exists where the sexually disturbing behavior results from brain damage or brain malfunction (e.g., fetishism and transvestism and other aberrant sexual conditions have been found to be associated with temporal lobe epilepsy [Epstein, 1961]). Sometimes libido may be reduced in individuals at certain stages of temporal lobe epilepsy. On the other hand, hypersexuality, though rare, may occur (Blumer, 1970). Sexual behavior may also be expressively distorted following brain injury (Weinstein and Kahn, 1961).
This is not to say that these conditions are significant in contributing to the incidence of obscene phone calls. In fact, Gebhard (1978) considers that a count of all sexual offenders whom he categorizes as “offenders with defects of intellect or thought processes” constitute only 10–15% of the offenders. He includes in this category persons who are retarded, brain damaged, psychotic, and seriously intoxicated (alcohol or drugs). Obscene phone callers in this grouping are only a tiny portion of that 10–15%.
Whereas in each of the above subgroups, the basic condition (retardation, brain damage, psychosis, intoxication) needs to be considered a priori to addressing the sexual problem, it is likely that intervention, where it is possible, may vary from condition to condition as well as person to person. It is with the group of sex offenders that Gebhart calls “normal” offenders that one can speak in more generic terms with regard to intervention strategies.
Given the very small number of obscene phone callers available for therapy at any given time, it is likely that therapy will be individual rather than in groups. Theoretically, they could be integrated into a group with persons with other sex deviancy problems, or in a group where the problems are not sex related. However, each of these approaches presents problems.
This writer does not endorse any particular style of therapy over another. There is merit to either psychodynamic approaches and there is also merit to behavioral treatments. Obviously there is also merit to an approach that combines both. In that obscene telephone callers have poor self-esteem and a need to express anger at women in a safe way, these are issues that psychodynamic treatment methods can modify. It can also impact on the area of interpersonal relations where this needs to be addressed. Insofar as generally, the obscene phone caller presents with a deviant sex style but with no typical psychopathology otherwise, one could just as convincingly argue that a behavior change is what is needed, and look to any of the many behavioral therapy variants for ways to work. It is likely that as with exhibitionists, recidivism is to be expected over time.
Psychodynamic therapies attempt to change the “inner person.” Where this occurs, overt problem behavior should no longer be necessary to the individual. Behavioral therapies change the action of the person. If the undesirable behaviors are eliminated, self-esteem ought to improve. The single most critical factor is the skill of the therapist built on experience, and the interest of the therapist in this particular problem.
Very little appears in the clinical literature (psychodynamic or behavioral therapies) that speaks exclusively to the experience of therapy of an obscene phone caller. There is a great deal that has been written describing and advocating particular treatment approaches to sexual deviates of all kinds. Perhaps the information on various styles of working with exhibitionists may be the most useful to the degree that there is similarity between both groups. There are good resources for an overview and particulars regarding assessment and treatment of exhibitionists (e.g., Cox and Daitzman, 1976). There are no similar volumes on the obscene phone caller. We have much yet to learn about this particular sexual deviancy.
References
Adams, H. E. and Chiodo, J. (1983). Sexual deviations. In Adams, H. E. and Sutter, P. B. (Eds.). Comprehensive Handbook of Psychopathology. New York: Plenum Publishing Corporation.
American Psychiatric Association. (1980). Diagnostic and statistical manual of mental disorders, (3rd ed.). Washington, D.C.: American Psychiatric Association.
Blumer, D. (1970). Hypersexual episodes in temporal lobe epilepsy, American Journal of Psychiatry, 126.
Brockopp, G. W. and Lester, D. (1969). The masturbator, Crisis Interventions, 1, 10–13.
Cox, D. J. and Daitzman, R. J. (1980). Exhibitionism: An overview. Exhibitionism: Description, Assessment and Treatment. New York: Garland.
Epstein, A. (1961). Relationships of fetishism and transvestism to brain and particularly temporal lobe dysfunction. Journal of Nervous and Mental Disorders, 113.
Freud, S. (1953). Hysterical phantasies and bisexuality. In Standard Edition, London: Hogarth Press, Volume 2, 51–58.
Gebhard, P. H. (1978). Sex offenders. In J. Money & H. Musaph (Eds.). Handbook of Sexology. New York: Elsevier North/Holland.
Gebhard, P. H., Gagnon, J. H., Pomeroy, W. B. and Christensen, C. J. (1965). Sex Offenders. New York: Harper and Row.
Hobson, W. F. (Dec. 1983). Objective of exhibitionists (in “Answers to Question”), Medical Aspects of Human Sexuality, 17, 91–92.
Kaplan,’ H. S. (Oct. 1974). Friction and Fantasy: No-nonsense therapy for six sexual malfunctions, Psychology Today, 8, 76–87.
Kinsey, A., Pomeroy, W., Martin, C., and Gebhard, P. (1948). Sexual Behavior in the Human Female. Philadelphia: W. B. Saunders.
Lester, D. (1977). Telephone counseling and the masturbator: A dilemma. In Bryant, C. (Ed.). Sexual Deviancy in Social Context. New York: New Viewpoints (Franklin Wattz).
Lester, D. (1975). Unusual Sexual Behavior: The Standard Deviations. Springfield, IL: Charles C Thomas.
Matek, O. (Fall/Winter 1980). Teaching volunteers of a crisis phone service to respond therapeutically to callers with sex problems, Journal of Sex Education and Therapy, 6, 24–28.
McGuire, R., Carlisle, J., and Young, B. (1965). Sexual deviations as conditioned behavior, Behavior Research and Therapy, 2, 185–190.
Mead, B. T. (June 1975). Coping with obscene phone calls, Medical Aspects of Human Sexuality, 9, 127–128.
Murray, F. S. (1967). A preliminary investigation of anonymous nuisance telephone calls to females, Psychological Record, 17, 395–400.
Murray, F. S. and Beran, L. C. (1968). A survey of nuisance calls received by males and females, Psychological Records, 18, 107–109.
Nadler, R. P. (1968). Approach to the psychodynamics of obscene telephone calls, New York Journal of Medicine, 68, 521–526.
Nadler, R. P. (1975). Obscene telephone calls. In Lief, H. I. (Ed.). Medical Aspects of Human Sexuality. Baltimore: Williams and Wilkins, pp. 283–284.
Russell, D. H. (September 1976). Obscene phone calls by women (in “Answers to Questions”), Medical Aspects of Human Sexuality, 10, 11.
Russell, D. H. (1971). Obscene telephone callers, Sexual Behavior, 1, pp. 2–7.
Sadoff, R. L. (1976). Other sexual deviations. In Sadock, B. J., Kaplan, H. L, and Freedman, A. M. (eds). The Sexual Experience. Baltimore: Williams and Wilkins Company.
Schwartz, M. F. and Masters, W. H. (1984). The Masters and Johnson treatment program for dissatisfied homosexual men, American Journal of Psychiatry, 141, 173–181.
Seeman, M. V. (May 1974). Obscene speech of psychotics (in “Answers to Questions”), Medical Aspects of Human Sexuality, 199.
Time. (May 9, 1983), p. 39.
Weinstein, E. A. and Kahn, R. L. (1961). Patterns of sexual behavior following brain injury, Psychiatry, 24.
Wrenn, E. (April-May 1985). Love among the chips, Campus Voice, pp. 33–38.
A Model of Sexual Aggression/Addiction{12}
Steven C. Wolf
Sexual aggression, i.e., acts of sexual behavior by one person against another without the benefit of that person’s informed consent, until very recently in the United States has been approached from very different points of view within the treatment and research community. However, an expanding body of objective data has begun to emerge which gives us a clearer picture of the nature of sexual aggression. Psychophysiological assessment has provided us with a better understanding of the arousal pattern and nature of arousal and motivation in the sexual offender. Specifically, it has been shown that individuals who act out in sexually aggressive ways do so as the result of the development of a sexual preference for that behavior, i.e., the child molester molests the child, in part, as a result of a developed pattern of sexual arousal towards children (Quinsey, 1979). This has given rise to further research into the repetitive nature of sexually aggressive behavior and it has been shown that individuals who are identified as having problems of a sexually aggressive nature are highly likely to have more than the single victim for whom they were identified and often to have additional victims both in that immediate sexual preference as well as other preference areas (Abel, Mittelman, Becker, Cunningham-Rather, and Lucas, 1983).
This article builds on this preliminary research to suggest a comprehensive model to in part explain the development and maintenance of sexually aggressive orientations. The data base for this paper is drawn from the research available in print in the United States, from clinical experience and ongoing research being conducted in our agency in Seattle, Northwest Treatment Associates (Wolf and Conte, 1984). This is a community based program whose single purpose is to treat adults who have been identified as acting out in sexually aggressive ways. Our clients are referred to us primarily from the criminal justice system as the result of some act of sexual aggression. As a community based program, our treatment acceptance criteria is based heavily on the individual’s presenting limited general pathology and his ability to, at least temporarily, control his behavior for a period of time sufficient for the treatment program to have made a significant impact in reducing the strength of his specific aggressive sexual orientation. That is, individuals who do not present histories of psychosis or schizophrenia and who, while chronic in their sexual behavior, are not compulsive to the point of being out of control. The result of this criteria is that the client population being treated in the community manifests less severe problems in terms of their personality and social competence and less sexually aggressive behavior than those found in inpatient settings or in a prison population. Our experience evaluating a broad spectrum of sexual offenders (over four thousand in the last twelve years) suggests that our clients are not different from other offenders in terms of structure of their behavior. Rather, they are different in the extent to which they have acted out their sexual attractions. As such, our clinical population represents an apparent skew in the direction of lower seriousness and lower intensity of aggressive orientation. The more serious individuals pass through our screening process and are referred on to a mental hospital or prison setting.
This paper will offer a theoretical model for understanding the origins and maintenance of sexual aggression. The hypothesis for this theoretic model is that there is a positive and increasing relationship between specific environmental/developmental experiences and the acquisition and maintenance of sexual aggression. This hypothesis describes a multidimensional model linking factors known to frequently occur in the lives of individuals identified as sexually aggressive with a learning model describing the relationship between inhibition and deviant arousal. This “holographic” model, as used here meaning the whole that is dimensionally greater than and three dimensional to its component parts, is based upon the belief that early experiences are seen as potentiators due to their influence on later attitudes and behaviors. Disinhibitors are transitory environmental factors or internal states that act to lower the person’s inhibitions against a specified behavior. These have an important role in weakening the inhibition (social controls) against and strengthening the attraction to sexually deviant behavior. The individual offender is seen as someone with a significantly disturbed developmental history who presents a personality profile consistent with a diagnosis of character disorder. These are individuals who present qualities of narcissism, distorted perceptions of the world about them, tendencies toward being ruminative, chronically depressed, and highly sexually preoccupied (Nichols, 1971).
Potentiators
At a reported rate of 47%, our population shows feelings of isolation within the family as a child. This is described by the offenders as a feeling of lack of closeness with parents and siblings. Family members questioned about this same quality typically describe similar feelings, although at a much higher rate. Also found are histories of violence in their family of origin, both with the offender as victim, 30% of the time, and as witnesses to physical violence, 36% of the time. They also report being victims of sexual abuse in 27% of the cases and victims of psychological abuse 24% of the time. Seventeen percent recall, as children, witnessing interfamily sexual abuse with some other family member as the victim (Wolf and Conte, 1984).
While accurate statistics for the general population are difficult, if not impossible, to derive, it appears that the experience of sexual and physical abuse by male children in the United States occurs at a rate of approximately 12%. For females this rate is approximately 25% to 30%. Based on these statistics, it would appear that our client population has experienced significant abuse and deprivation in their family of origin at a rate approximately twice that of the general population.
The inference to be drawn from this is that the abuse/isolation experience increases the individual’s potential for developing problems of sexual aggression in adolescence and adulthood. It also appears that this potential seems to increase in a direct relationship to the amount and seriousness of the abuse experienced. For example, when one looks at offenders along a continuum of increasing levels of seriousness and frequency, one finds increasing rates of sexual victimization in their childhood (Groth and Longo, 1982).
Personality
These potentiators seem to have a direct impact on the form of the adult personality. Psychometric assessment of this population using the MMPI (Minnesota Multiphasic Personality Inventory) reveals elevations on clinical scales suggestive of the diagnosis of character disorder. Specifically, elevations on scale four, psychopathic deviance; scale eight, schizophrenia; scale seven, psyesthenia; and scale two, depression. There is also a tendency for significant elevations on the K scale (Nichols, 1971). The interpretation of these elevations is that they point to individuals who are prone to acting on their impulses, which are frequently manifested in the areas of alcohol or drug abuse, sexual promiscuity, or physical aggression. They show low frustration tolerance and poor social adjustment. They are also described as tending to be rebellious and show an inability to anticipate the consequences of their behavior. They tend to form interpersonal relationships quickly which are shallow and lacking in true intimacy. They show a strong tendency to project blame for whatever current difficulties they may be experiencing. They are also frequently described as lacking in empathy or in deep interest in other individuals, as feeling socially alienated from both the world around them and from their families, misunderstood and isolated, and who frequently compensate for these feelings through need-fulfillment fantasies. They are also individuals who are generally dissatisfied with their situation in life and tend to be high strung and worrisome or ruminative in their thinking (Nichols, 1971).
Following closely on these MMPI descriptions are our clinical observations that these individuals tend to be narcissistic, exhibit many schizoid qualities including distorted perceptions of the world around them, tend to be ruminative, chronically depressed, and sexually preoccupied.
In terms of sexual preoccupation, we have observed that these individuals have developed a coping strategy for dealing with internally felt stresses wherein they escape to sexual fantasy and behavior. For example, it is frequently the case that external stressors precede their recourse to aggressive outlet. In this regard they seem to use sexuality in a self-medicating manner, much in the style of an alcohol abuser’s use of that drug. For example, clients report feeling the desire and/or need to masturbate prior to stressful situations such as meeting with their boss, delivering a presentation or speech, or to relieve the general internal pressure that they experience as a result of problems within their families. Reoffenses while in treatment are most often preceded by high levels of internal stress in the client’s environment which manifests itself in increased sexual ideation and acting out. One of the “warning signs” of which we advise our clients’ families is any change in the client’s sexual frequency, talk, use of pornography, etc.
Sexuality, as a stress-reduction mechanism, can be understood as a learned “weak membrane” response. That is, when under stress, their responses will include using sexuality to self-gratify and to avoid dealing with the attendant stressor. This functions rather like squeezing the outside of a balloon which has a weak point on its skin. The local weakness is the area which will give first under pressure. The sexual offender, under pressure, will give first in the weakest area of his personality “membrane,” i.e., the most frequently exercised area of his personality, i.e., sexuality (Smith, 1980).
Disinhibitors
Disinhibitors are factors which act to disrupt the individual’s normal social controls (inhibitions) against sexual aggression. They also have a role in terms of justification or rationalization which serves to further the individual’s development and continuation of their sexual deviance. They exist within the environment in which the sex offender lives. They are situations which serve to facilitate the development of the aggressive behavior pattern. For example, in understanding an incest offender, one looks at the quality of the interpersonal relationship between the offender and his spouse, his relationship with his children and his overall level of interpersonal relationships with people both in and outside of his immediate family. One looks for qualities which would serve to isolate him and a particular family member and to weaken his inhibitions against, for example, sex with his child.
When one observes an individual who has in his developmental history experiences of sexual or physical abuse, a sense of interpersonal isolation in his family of origin and other Potentiators, one would expect that he would enter adolescence and/or adulthood with a lower baseline of resistance/sensitization to deviant attractions. If he has grown up “knowing” that adults can be sexual with children without consequences for that behavior, even when the children do not like what is being done to them, he has learned a significant lesson about the differences in roles between adults and children. This sort of psychopathic understanding tends to decrease the offender’s resistance to deviant attractions as it provides direct evidence that sex with children, for example, is possible (Yates, 1984). The same argument could be made that these environmental exposures to aggression function as a model that teaches the individual that sexually aggressive behavior patterns are acceptable coping responses to specific stresses within the environment (Bert, 1983).
Sexual Fantasy
Whatever the cause, it seems consistent in clinical experience that men who are identified as sexual offenders have early on developed a pattern of sexual awareness of and attraction to sexual aggression. This awareness and attraction is usually expressed first in masturbation fantasy, i.e., a repeated pattern of ideation used for any form of sexual gratification up to, but not necessarily including, ejaculation. This masturbatory fantasy seems to perform three functions. First, it acts as a disinhibitor toward the behavior fantasized about. Second, it reinforces the attraction toward the behavior which is the focus of the masturbatory fantasy. And third, it reinforces the rationalizations and justifications used in the fantasy which is the focus of the masturbation.
In terms of its disinhibiting quality, it would appear that it functions very much as a systematic desensitization model in which a phobic sensitization to some object or behavior is reduced through repeated pairings of the phobia with a relaxed or otherwise aroused state. For example, the masturbatory fantasy systematically and repeatedly brings the individual face to face with the behavior in a safe, comfortable environment wherein he is also experiencing a high level of sexual arousal. In this respect, sexual arousal performs the same function that reciprocal inhibition performs in systematic desensitization. That is, even if the sexual behavior is believed to be forbidden to the individual, when he fantasizes about it and begins to experience the sexual stimulation and gratification, this will in time, with enough repetitions, desensitize him to the sense of taboo that the behavior brings with it (Wolpe, 1958). At the same time, the consistent repetition of the aggressive theme in association with the pleasant sensations of sexual arousal and/or ejaculation, serves to reinforce the attraction to the aggression so that the overall arousal and attraction to the aggressive focus increases (McGuire, Carlisle, and Young, 1965; Skinner, 1953).
In effect, as illustrated in Figure 1, we have two intersecting learning curves. On the one hand, the disinhibition (descending) curve and, on the other hand, the aggressive (ascending) curve. Beyond the point at which they cross, the inhibition against the aggressive focus is lower than the attraction to the aggressive focus and the probability for the behavior occurring in reality is greatly increased.
At the same time that this is occurring, the person is also having to deal with the sense of guilt or embarrassment that he experiences post-ejaculation, or post-sexual stimulation when he is confronted by the reality of what he is either doing in actuality or wanting to do in sexual fantasy. With repetition, the individual begins to incorporate into his fantasy a pattern of realization and justification which further disinhibits him and desensitizes him to the taboo nature of the behavior. It has been observed in clinical interactions that the fantasies of sexual offenders contain emotional escape clauses. That is, within their rationalizations there exists a structure of excuse and permission-giving that makes them somehow not responsible for their own behavior. They will, for example, in fantasy tell themselves that this is not sexual abuse or molestation, that it is sex education or that somehow the victim wanted it or that they only did it when they were intoxicated or tired, asleep, etc.
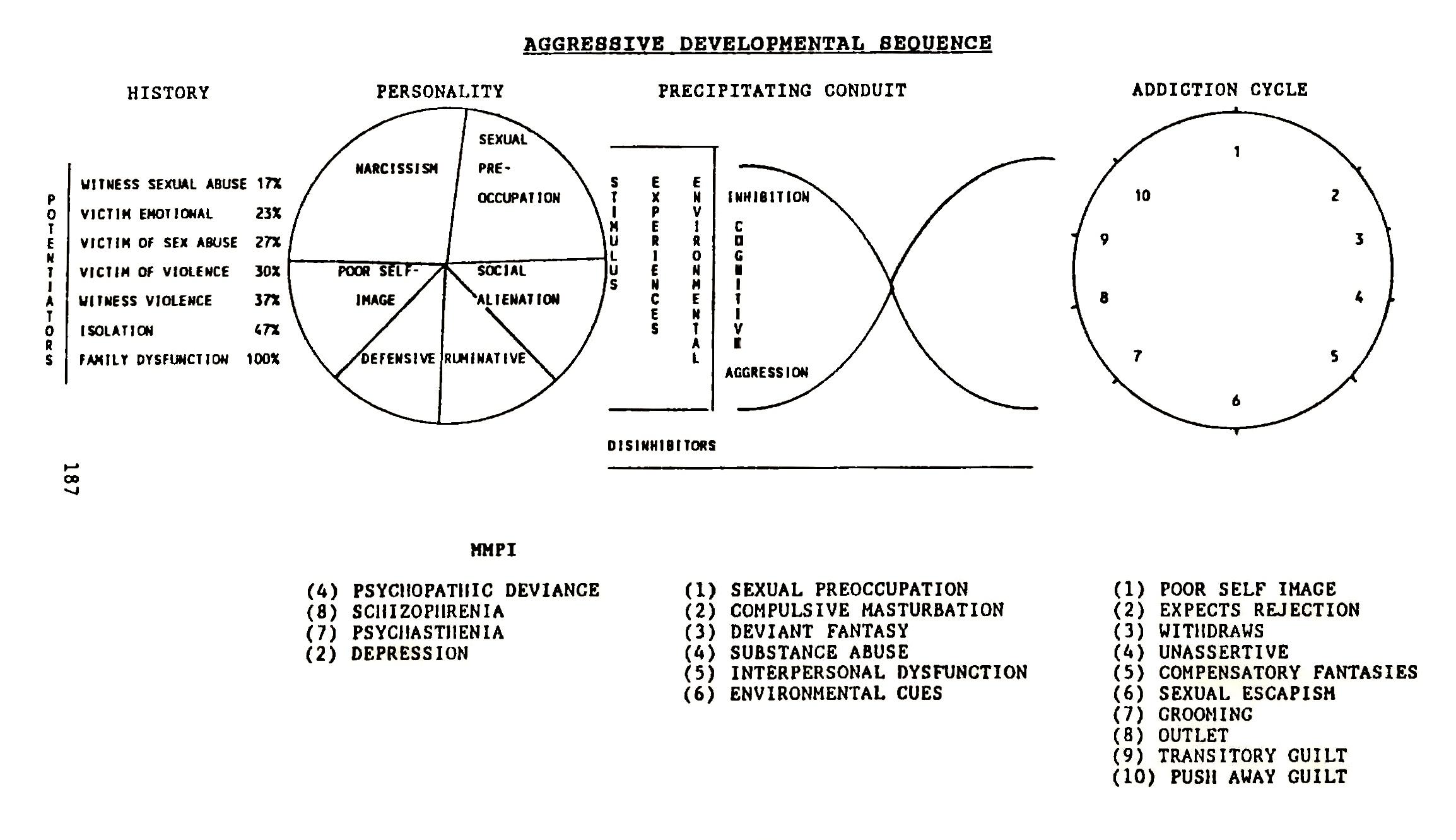
This constant process of disinhibition and reinforcement tends to control the level of anxiety that the individual might otherwise experience with the recurrence of this kind of aggressive fantasy and/ or behavior. The behavior fantasized about also changes over time as a result of this process. Typically, one finds a pattern of the offender reaching to achieve in fantasy more sexual gratification or more fulfilling sexual behavior than they have achieved in reality. Additionally, as they desensitize themselves to these increased levels of sexual acting out, their level of arousal and comfort with it allows them to expand and explore further areas of sexual behavior. It is this quality of sexual fantasy that leads to the belief within the offender’s personality structure that the “next time will be just a little better.” This seems to move the offender forward toward additional sexually aggressive behaviors, one small step at a time. As such, one sees a pattern of progression of the behavior in offenders’ histories. While this progression may be very slow and the change may only be observed over long periods, it typically exists within their pattern.
One must not overlook, however, the strength of the offender’s belief system that what they say they will do or won’t do again in relationship to their deviant acting out is something that, at that exact moment, they wholly believe. In terms of their promises to, for example,.“not do it again,” this serves to relieve them of any sense of guilt or fear of the continuing problem. If you will allow me a personal observation, I know from my own life as a perpetual dieter that I start each day in much the same manner. I see myself full length in the mirror and recognize the need for a significant weight loss. At that moment, I promise myself that from this time forward I am on a strict diet and will eat sensibly so that I can return my physical self to the prime specimen that I know myself to be. However, by lunch time my good intentions and the embarrassment of seeing myself for what I truly am have begun to fade and the desire of my hunger begins to supplant it. Further, there is always that escape clause in the back of my mind that says, “Well, I’ll have a good (read in large) lunch and then I won’t do it again.” That, of course, is my code for I’ll eat sensibly at dinner. My mistake is failing to learn that there is always another meal (attraction/ need) and that I will always be just as hungry again (aroused) and I, like the sex offender, quickly forget the powerful drive state of the hunger (sexual) need. In this way I doom myself to repeating the behavioral cycle again and again. Similarly, the sex offender, after the point of ejaculation or decreasing sexual gratification, believes that there is no next time and that they will never be out of control again.
Addiction Cycle
Upon close examination of both present behavior and the patterns of behavior established historically by the sex offender, one begins to see a predictable cyclical pattern to their acting out (see Figure 1). In charting this addiction cycle, we start at a point described as “Poor Self-Image” because it appears to be the entry level or baseline status for the offender in terms of a constant emotional undercurrent of depression or dissatisfaction with his or her life situation. These clients present an historical pattern of depressive ideation as a response to felt stressors. This seems to be even more the case when the felt stress is interpersonal in origin. Whatever the case, it seems this leads them to expect that others would reject them personally “If they only knew what I was really like,” i.e., about their sexual behavior, developmental histories, etc. This expectation of rejection, as a response to the pressured poor self-image, exists as a manifestation of the basic conflict between their internal expectations for themselves and the reality of themselves that they see.
Given their history of poor interpersonal skills and superficial relationships, it can be understood how and why this pattern of withdrawal in response to stress and fear of rejection develops. Sexual offenders seem to compensate for the sense of isolation through need-fulfillment fantasies. With the sexual offender, these fantasies most often take on a sexual tone. This escape to sexuality can be understood as a learned coping mechanism which develops fairly early in their lives out of a realization that sexual self-gratification is a way of displacing other more unpleasant emotional feelings. The fantasy serves as a cognitive rehearsal of aggressive behavior in which fantasy serves to increase their attraction to the fantasy behavior and, if the fantasy is fixed on a specific behavior or individual within their environment, to increase their need for or attraction to that individual or that behavior. The result is that the fantasy begins to “groom” the environment. That is, because of the increased attraction for the behavior or the person, the offender begins to expend increasing amounts of energy on being close to and involved with them. And, if the focus is another person, their attraction behavior stimulates and reinforces that person’s desire to be around them. In this way, the result of the fantasy pairing is to create an atmosphere in which the target of the sexual fantasy is also “groomed” to be around the offender.
At the same time, the environment tends to greatly influence (groom) the structure of the offender’s fantasies. If, at least based on clinical observation, these individuals tend to be very concrete and primitive in their thinking, attitudes, and beliefs, they are most likely to become fixated sexually with someone or something within their immediate environment. Someone or something who at least in some way seems attainable to them. In that light, the environment plays a significant role in shaping the early stages of their fantasy behavior, then continues to affect the structure of the fantasy in terms of environmental cues, availability, times, etc.
In close proximity to this expression of sexually aggressive preference, especially if this behavior is followed closely by ejaculation, these individuals will experience a “return to senses” and be faced with the^ reality of what they have done. They will feel both fear of being caught as a result of their sexually aggressive behavior or embarrassed by the wrongness of it. They will feel levels of guilt ranging from mild to extreme for a brief period of time. Brief, because characterologically these are individuals who do not generally take responsibility for themselves or their behaviors. The tendency is to direct responsibility outward or to, as quickly as possible, lower their sense of responsibility by, for example, promising to “never do it again.” Additionally, because characterologically they do not learn from their mistakes, they will believe their own assertions that he will indeed never do it again and will be able to quickly forget about it because, in their words, “What’s past can’t be changed.” All of this is part of what we see as the process of “reconstitution.” That is, returning the individual to his original emotional state. The problem is that even though the individual recognizes that he has failed again, because he cannot cope with his own sense of guilt, he must deny its existence and at least on a primitive level, believe that he will not reoffend. Individuals are, thus, left again with a continuing and increasingly unresolvable conflict between their expectations of themselves and reality. The result is an increasingly damaged self-image and reinforced pattern of depressive ideation and poor self-image.
Behavioral Progression
It is this same quality of disinhibition to behavior and failure on the part of the offender to recognize the cyclical and repetitive nature of his addiction that also seems to make him more susceptible to the acquisition of further types of aggressive focus. For example, both in research and in our clinical experience, it has been observed that when one looks deeply into the backgrounds of the identified sexual aggressive, one typically finds more than one type of sexual acting-out (Abel et al., 1983). It is quite possible that this is the result of the disinhibition process, in that, once a person is disinhibited to and aroused to one particular focus of sexually aggressive behavior, it is significantly easier for them to acquire a second or third or fourth focus. This is much in the same manner that it would be easier for a skydiver to take up hang-gliding than it would be for someone who is not disinhibited to heights.
This is even more true of the offender who has experienced sexual or physical abuse as a child. The knowledge that adults can do whatever they want, seemingly without consequences, is a powerful act of permission giving in the offender’s value and belief system. The end result is that the attraction for the behavior increases in the presence of the permission given by this psychopathic insight about adult behavior.
Structure of Sexual Fantasy
In terms of the general structural flow of fantasies of adult sexual offenders, one again finds similarities in that the fantasy will precede from some form of recognition of either a potential victim or potential situation through active fantasy which includes qualities of recognition, assessment, justification, planning, and execution of the aggressive behavior (Figure 2). Specifically, the recognition will include qualities of the antecedent behaviors taken from the individual’s environment such as being highly stressed, depressed, feeling isolated, or being alone with the victim. It progresses through recognizing the victim as a potential sexual partner which includes the client’s own justifications of this recognition from his perceptions of the victim’s behavior. These perceptions (distortions) give him permission to act out sexually. For example, upon seeing an adolescent child on the street, an offender with that particular sexual preference may look at the child and justify his attraction to them by saying to himself, “If they didn’t want me to look, why do they (a) wear tight blouses, (b) wear tight pants, (c) wear their hair cut that way, or (d) use makeup.”
The next element, the storyline, involves the offender in more active fantasy about the component parts of his potential victim’s body, i.e., being attracted to face, breast, buttocks, legs, etc. and expressing a sense of curiosity about what they might feel like, look like, etc. The next phase has the offender moving into a state of readiness and concocting a plan for action. For example, turning to the preadolescent or adolescent on the street and thinking, “If he or she is hitchhiking, then I could pick them up.” Hitchhiking here being justification for the behavior and permission to act it out. After all, in the offender’s words, “If he or she is hitchhiking, they are sexually available.” If the environment duplicates the fantasy, that is if the potential victim is indeed hitchhiking, the offender moves to the next phase and offers the individual a ride. Now the offender has isolated his potential victim and he moves into the execution stage of sexual fantasy, beginning to feel aroused, excited, nervous, or whatever words the offender uses to describe his state of sexual arousal.
At all points along the fantasy continuum, the offender is justifying and rationalizing his behavior, thereby desensitizing himself to whatever social inhibitions might otherwise interfere with his carrying out his plan of action. This pattern has shown itself, in our clinical experience, to be the same regardless of the offense type or the history of the offender. Again, it is not so much how the offenders are different in the style and structure of their fantasies, but rather how they are the same. In any case, once a continuing pattern of sexual acting out is established, the sexual preference cannot be “talked out of” the offender. Other more direct means must be found to alter the deviant patterns of arousal. This is true for virtually all repeat sexual offenders, including incestuous offenders. They share the same general historical and behavioral characteristics that child molesters manifest, including a clear pattern of arousal to children (Wolf and Conte, 1984). They, for example, will begin to recognize their child as a possible sex partner, begin to justify and reinforce their attraction with fantasy, frequently of themselves as the unwitting victim of the child’s sexual aggression or their wife’s rejections. As their interest in and sexual arousal for the child increases, they increase their interaction with the child, thus beginning to isolate the child from the rest of the family, and increase the probability that the offender will be able to be sexual with the child without the child’s having anyone else to turn to.
Clinical Implications
Research and clinical experience suggests that individuals identified as sexual offenders are individuals who are acting on a clear pattern of sexual preference. This pattern of behavior, once established, is chronic in nature and incorporated both as a result of and as part of the person’s personality structure. With the development of one pattern of aggression, others are likely to develop. These qualities point to the need for thorough and comprehensive assessment of the sexually aggressive individual along very specific lines. It should also be clear that the sexual offender’s self-report is not adequate for this task. It is highly unlikely that any person identified as a sexual offender will, without some outside pressure, reveal the true nature of his or her sexually aggressive, illegal, and inappropriate behaviors to a therapist who is a stranger to them and frequently seen as a potential threat to their freedom. As such, any form of comprehensive assessment of this individual has to include a review of all data available including victim statements, witness statements, attendant assessments of the offender by their therapist or by family members or friends or co-workers, etc. Increasingly, it also includes psychophysiological assessment involving instruments such as the penile plethysmograph (Zuckerman, 1971) and a clinical polygraph. It means assessing the person’s developmental history for clues to the development of the person’s personality as examined using instruments such as the MMPI. This also means assessing their past and present environment and behavioral response patterns in order to understand the problem as it exists now.
When one has completed this kind of comprehensive assessment of the sexual offender and understands the historical perspective as it applies to personality and environment, one then has a structure from which one can plan for treating the specific patterns of the offender’s sexual arousal/addiction. For example, working with the offender to recognize the existence of distortions in his attitudes, beliefs, and values (personality) and the role they play in creating and justifying his aggressive behavior. Also working with him to recognize the role of his own childhood experiences (Potentiators) in creating these attitudes, beliefs, and values. Next, working with the offender to recognize the cyclical/addictive nature of his aggressive behavior including recognizing it and understanding the role of his personal disinhibitors in the maintenance of his sexual aggression. Finally, working with the offender to recognize and inhibit his deviant sexual behavioral preferences.
The above represents a number of different areas of therapeutic concerns, each with its own therapeutic approach. At our agency, \Ve use a combination of confrontive group therapy, “traditional” insight talk therapy, family therapy, couples therapy, and cognitive behavioral counterconditioning and aversion therapies to address these needs. In each case we work to establish the developmental sequence of the sexual behavior, work to inhibit or make aversive the aggressive arousal and to strengthen the offender’s interpersonal skills and values. This comprehensive approach has shown itself very effective in lowering the client’s level of aggressive arousal, as measured by the penile plethysmograph and polygraph. It has also shown a good level of success in limiting their return to sexual aggression. Flowever, this is still an experimental approach. Long term results (beyond ten years) have not been observed.
Based on this model, treatment of this population is neither easy nor rapid. It means in a very real sense oftentimes extensive reparenting of the individual offender to ameliorate the influences of Potentiating Factors. It means working with him and his family or extended family in restructuring their attitudes and beliefs about men and women, about adults and children, and about sexuality to provide a more appropriate/nonabusive atmosphere in which they can live.
It is hoped that this theoretical model will be of some utility to the treatment community in assessing and working with this difficult and dangerous population. Additional research is certainly needed in the area of personality assessment as well as psychophysiological assessment of identified offenders and identified “normals.” It also seems important that we begin to look more closely at victims in terms of the impact of this behavior on nonoffended as well as offended family members. This is especially true in terms of the impact of this kind of experience on male children, since statistically they are the most likely to grow up and become offenders themselves. Further exploration in the area of values and attitudes acquisition of children and adolescents would also seem to be a fruitful area of research. Finally, efforts must be made by clinicians to keep and share data, through published articles, their experience and data gathered from their work with clients. It is hoped that the model presented will be of some assistance in generating that kind of cooperation and further research.
References
Abel, Mittelman, Becker, Cunningham-Rather, & Lucas. (1983). The characteristics of men who molest young children. Presented at the World Congress of Behavior Therapy.
Bert, M. R. (1983). Justifying personal violence: A comparison of rapists and the general public. Victimology, 8, 131–150.
Groth, N. & Longo, R. (1982). The sexual assault of males: Victims and offenders issues. Fourth National Conference and Workshop on Sexual Aggression.
McGuire, R. J., Carlisle, J. M., & Young, B. A. (1965). Sexual deviation as conditioned behavior: A hypothesis. Behavior Research and Therapy, 2,1985–90.
Nichols, H. (1971). Effects of treatment as measured by the Minnesota Multiphasic Personality Inventory. Western State Hospital. Ft. Steilacoom, Washington.
Quinsey, V. (1979). Sexual preferences among incestuous and nonincestuous child molesters. Behavior Therapy, 10, 562–65.
Skinner, B. F. (1953). Science and human behavior. New York: MacMillan Company.
Smith, T. A. (1980). Weak membrane theory. Northwest Treatment Associates, Seattle, Washington.
Wolf, S. & Conte, J. (1984). Characteristics of sexual offenders in a community treatment program. Unpublished.
Wolpe, J. (1958). Psychotherapy by reciprocal inhibition. San Jose, CA: Stanford University Press.
Yates, E., Barbaree, H. E., & Marshall, W. L. (1984). Anger and deviant sexual arousal. Behavior Therapy, 15, 287–294.
Zuckerman, M. (1971). Psychological measures of sexual arousal in the human. Psychological Bulletin, 75, 297–339.
A Treatment Model for Sexual Aggression{13}
Timothy A. Smith
Roger W. Wolfe
The utilization of Aversive Behavioral Rehearsal has been primarily reported by Wickramasekera (1972, 1976, and 1980). In the most extensive article to date (Wickramasekera, 1980), twenty-three chronic exhibitionists are followed for periods up to nine years. One reoffense by one individual is reported. To those having extensive experience working with exhibitionists, these success rates seem quite high. Exhibitionism has been noted to be one of the most difficult and recalcitrant of all forms of sexual paraphilia to successfully control. However, at least three other clinical investigators have reported like results using similar procedures to those outlined by Wickramasekera (Jones and Frei, 1977; Reitz and Keil, 1971; Serber, 1970; Stevenson and Jones, 1972). All of these studies utilized exhibitionists as subjects. It could be argued that exhibitionists represent the prototype of sexual offenders and that whatever will work for exhibitionists will work for other types of paraphilias. In addition, exhibitionists lend themselves readily to research given that they typically will have high frequency patterns and relatively long-term histories before they reach a treatment setting (i.e., the thirty-two exhibitionists in our sample had a mean of over two thousand separate offenses). Typically, if these individuals are going to reoffend, they will reoffend in relatively short order. Results become evident with follow-up periods of several years duration.
The present authors have taken the procedures outlined by Wickramasekera and modified them for ease and enhanced economics of application. The procedure has been modified to utilize it in the treatment of other paraphilias as well. In fact, of the one hundred forty-four subjects on which outcome data will be presented, only thirty-two are exhibitionists.
There are three major modifications which have been instituted in this procedure. The first one is the elimination of the “audience.” Wickramasekera’s (1980) procedures call for an audience of three females and two males. They were drawn from the staff at the community mental health clinic where he practiced. The present authors function in a private practice setting and felt the logistics and economics of gathering six professionals in one room to be cumbersome and difficult, not to mention the added expense of professional time. The present protocol involves just the therapist and the client, although others (group members, significant others) are brought in to view videotape replays of the sessions. The second major modification is the elimination of full nudity. Frankly, this modification was done for public relations purposes. Most of our clients are involved in the criminal justice system and even though a rational argument can be made for the utility of full nudity in this procedure, it was felt that both community acceptance and client acceptance level would be enhanced by substituting simulated nudity, wherein, in the sections where nudity is called for, the client is seen in flesh-colored pantyhose with a plastic simulated penis. A third departure from the Wickramasekera (1980) protocol involves the use of department store mannequins as victims. Mannequins have previously been used for the assessment of sexual offenders and it was found that interacting with a “human-like” figure elicited behavior not previously reported by the offender (Forgione, 1974). Mannequins of male and female children as well as adults were selected to make treatment available to pedophiles and other hands-on offenders as well as to provide targets for exhibitionists.
Subjects
The subjects are one hundred fifty-four sexual offenders who were consecutively offered the opportunity to participate in Modified Aversive Behavioral Rehearsal (MABR) commencing in 1981 through January of 1985. The subjects range in age from nineteen through sixty-three with the mean age being approximately thirty-seven. Nearly all subjects had previously been involved in our treatment program for a minimum period of six months. A breakdown of the primary offense behavior patterns is presented in Table 1. Subjects displayed vaiying histories of deviant behavior. Most of them would be classified as relatively chronic offenders. A breakdown of the average number of victims per client is also presented in Table 1.
Protocol
Modified Aversive Behavioral Rehearsal
Phase 1 — Preparation involves the therapist overtly and covertly engaging the client to the point that he requests that he be given this very powerful, often humiliating, treatment.
Phase 2—Active treatment systematically elicits and punishes all of the client’s offending behaviors and fantasies. It creates tremendous cognitive dissonance within the client as he perceives his deviance as it really appears for the first time. This phase requires three weeks of effort and discomfort with no reward for the client. It offers a realistic in vivo punishment of compulsive behaviors.
Phase 3 — Public Self-Disclosure — the client, therapist, and significant other(s) (wife, closest friend, relative, treatment group) view the client engaged in his deviancy. He no longer has a “secret”; denial of any aspect of his deviancy becomes useless. It requires risk-taking and becoming truly public with his deviancy.
Phase 4-Follow-Up and Vicarious MABR. The client’s videotape is used for follow-up sessions with his therapist at regular intervals. Frequently, it is shown in his group setting and he sees other clients’ tapes. The viewing of a tape is an aversive experience and clients (other group members), who have not been filmed, report strong emotional reactions. The client knows that he has a permanent “public” record of himself as a deviant in his therapist’s office. Extended follow-up will be undertaken to determine the impact of this knowledge upon the client. Initial follow-up (six months) reveals that clients do not become comfortable; their behavior continues to suggest aversive emotional states.
Table 1: Outcome of MABR “Acceptors”
After a Mean Two-Year Follow-Up Period
| Offense Behavior | Number | Reoffend | % Known Reoffenders | Mean # < Victims | |
| Heterosexual child molester | 88 | 2 | 2 | 4.5 | |
| Exhibitionist | 32 | 5 | 16 | 2012.0 | |
| Obscene Phone Caller | 1 | 1 | 100 | 100.0 | |
| Voyeurs | 5 | 1 | 20 | 260.0 | |
| Homosexual child molester | 15 | 0 | 0 | 23.0 | |
| Female homosexual child mplester | 1 | 0 | 0 | 13.0 | |
| Child rapist | 2 | 1 | 50 | 3.0 | |
| Adult rapist | 1 | 0 | 0 | 5.0 | |
| Breast grabber | 2 | 1 | 50 | 100.0 | |
| Bisexual child molester | 11 | 0 | 0 | 9.0 | |
| Cross dresser/panty fetish (steals clothing) | 1 | 1 | 100 | 50.0 | |
| Total | 144* | 7* | 5% |
| Mean Follow Up | 24 Months |
| Range Follow Up | 1–45 Months{14} |
Treatment Procedures — MABR
The following describes in detail, treatment techniques for the application of MABR with pedophiles and exhibitionists.
Phase 1 —Preparation
The goal of the preparation phase is to prepare the client, inform the client, and elicit his apprehensive participation. It should be conducted one week prior to beginning the treatment sequence.
The client is told about the power and effects in absolute terms. “This technique is extremely powerful and appears very effective ... it is different than any other type of treatment we offer here.” Various technical aspects can be discussed such as the need to punish all aspects of an offense sequence and how MABR facilitates this, etc. The therapist should then methodically, painstakingly inform the client of the possible side effects, the voluntary nature of the treatment and the hard work involved.
Covertly the therapist sets the stage that a very profound, powerful experience is available, but the therapist has genuine concerns about the client’s ability to tolerate the experience. The various forms, releases, contracts, and the videotape technology all serve to reinforce the image of a power that must be carefully controlled.
Once the client asks to begin the technique, the therapist insists that a week be spent contemplating his decision. He is urged to read the information sheet and to discuss the procedure with his wife or significant other.
Individualized treatment plans are negotiated (all subject to approval later) and initial choices of mannequins, clothing, apparatus, etc. are discussed.
Phase 2—Active Treatment
Session 1 —Pedophiles and Exhibitionists
The client returns and reaffirms that he wants the treatment. The therapist insures he understands all the implications of his decision. He is asked to sign the forms. Discussion of other issues (group, family, etc.) is sternly discouraged by the therapist. (There is serious business to be about here!)
Thirty minutes of reliving actual offending takes place with no mannequins present. The client speaks in present tense, just as he thought and felt during offending. “I’m looking at my son, Bill, I can tell that he wants me to fondle him again, the way he walks by tells me” ... “I’m getting into bed with Sue —she’s quiet so I know she wants me to rub her all over.” The therapist assumes the “naive observer” role and forces the offender to elaborate in exhausting detail who and why he is molesting or exposing to. For example:
Th: Well, what are you doing walking down the hall to your daughter’s room?
Cl: I’m turned on and going to try to molest her.
Th: :What? She’s your daughter!
Cl: I know, but I think she wants it.
Th: You’re 40 and she’s eight; how can an eight year old want sex from her father?
Cl: I figured she did because she didn’t tell the last time.
Th: You mean you’ve actually done this before!
Cl: Yes—for about three years.
Th: God! You must hate this child.
Cl: No, no I love her!
Th: What are you doing now?
Cl: I’m laying on her and humping her and trying to get an erection so I can screw her ...
The therapist should focus his attention to the monitor and not engage the client who will be desiring validation that he is no longer liking the role he is playing.
Following filming, the therapist silently plays 5–10 minutes of the film. He again speaks of the possible side effects, how to deal with them, and reassures the client that he has done well—that he is on the right track, etc.
Session 2-Pedophiles
The client interacts with a victim (mannequin) present, but does not touch the mannequin. With the therapist probing and questioning, again as a naive observer who is appalled by what is happening (it’s helpful to visualize someone you know who is not in this field and not desensitized and model their responses), the client describes his distortions and offenses.
The emotional intensity of the session increases substantially with the presence of the mannequin, and clients may “escape” or disassociate themselves. Therapist probing and questioning of physical details of the victim and the setting help to control this escapism.
Repeating his distortions, excuses, grooming, and control statements verbatim, the client describes the whole offending sequence speaking to the mannequin. Educating the naive therapist, the client eventually forcefully and frustratedly argues that he planned, controlled, and abused his victim, frtuch to the dismay bf thé óbserver. Skillful camera work focusing on the mannequin during physical description distortions greatly enhances post-session viewing. Many clients will become involved with the mannequin. They will emotionally relive the pre- and post-phases of the abuse and some report that they felt physically nearly the same sensations that occurred during molestations. The therapist should be alert to these possibilities and flexible enough to depart from format and merely film the client on these occasions. This footage will be beneficial to the client in post-session viewing. Following Session 2, the therapist should plan for more debriefing and reassurance for the typical client will be very distraught.
Session 2—Exhibitionists
A standard second session for an exposer or peeper will be more accelerated than the pedophile sequence described previously. In this session he will “expose” in a previously agreed-upon manner to a mannequin or out a window, in a symbolic car, etc. The client talks his way through his entire pattern while the therapist acts naive, much as Session 2 pedophiles describe. Since many exhibitionists follow fixed sequences, it is possible to be able to focus in detail on each step of the offending pattern.
The client may be in running shorts or swim trunks under flesh-colored pantyhose, and utilize a plastic simulated penis where called for. Once negotiated, a given exposing condition should not be discarded while in session.
In addition to the naive questioning, a therapist may use interventions such as normal conversation to maximize the aversion. For example, a client will be simulating exposing from his car and masturbating to women while on the street; the therapist can engage him in conversation about his plans and goals, his occupation, etc. This incongruity is very punishing, both during the session and in Session 4 viewing.
Session 3-Pedophiles
During this session, the client directly, physically, sexually assaults a mannequin. The treatment goal is to re-enact the behavior in an aversive environment.
Preplanning includes having the client provide typical clothing, such as a bathrobe, and any peculiar physical setting, e. g., couch, chair, bedroom, should be replicated as closely as possible.
The client and therapist select the behaviors to re-enact and the client is instructed to combine all the verbal sequences from the previous sessions and then physically assault the mannequin in exactly the manner he actually offended.
The therapist begins supportively and cautiously encouraging the client to re-enact the offense. Progressively he becomes more sarcastic, obnoxious, and decidedly deviant. He drives the client to reenact the offense; he repeats the client’s rationalizations and distortions, e.g., “Look at the way she is sitting, you know she wants it!” He exhorts the client to verbalize the thrill and pleasure he is getting and encourages him when he does.
Some clients show great resistance and refuse to participate at this point. The therapist increases the pressure, arguing dramatically that the client really wants to offend; that he has built his life around it, and further details about how much the victim obviously wants it. Often these impasses end with the therapist arguing that the client really wants to offend and the client emotionally pleading for the right of the mannequin not to be victimized.
Other clients show astonishing willingness to re-enact their offenses. These clients may be very highly motivated, or may not be feeling punished by the situation, still believing some of their distortions, etc. This is a more likely event when the technique is used early in treatment (see timing section).
When the client does not appear emotionally impacted, the therapist can employ several technical modifications. He may remain calm and simply allow the client to be blase about the abuse, thereby filming a “real” picture of where the client is in his treatment progress for use in evaluation and confrontation. Alternately, he may exhort the client to act out his fantasies of sexual activity with the victim. Often these are more abusive than what he actually did and this usually provides enhanced impact. The client should speak to the mannequin, telling her/him what he has really wanted to do, and next act out those fantasies. This procedure appears more therapeutic when the client is asked spontaneously to agree to work on fantasies. Preplanning will usually result in denial and minimization of fantasy material.
Session 3—Exhibitionists
This session focuses on fantasy material exclusively and is flexible according to individual client needs. The fantasy experience of exhibitionists is a critical element in the maintenance of their deviant behavior and, as such, it needs to be re-enacted in a dramatic, yet aversive, way.
The therapist is again a driving, deviant force in this session as he exhorts the client to act out his ultimate fantasy with the victim.
The client finally achieves his fantasy, e.g., that of a woman actually standing still and allowing him to have intercourse with her, but when he recreates the behavior, he feels humiliated and punished.
Considerable preplanning and treatment work is necessary before the therapist can reasonably feel confident that the client is acting out his actual fantasies.
Phase 3—Public Self-Disclosure
This session is devoted to the objective of client self-disclosure that is unavailable through verbal report. At great self-risk the client asks the most important person(s) in his life to view him as an offender. Distortion and denial are no longer of any use as his wife sees him planning, grooming, controlling, and molesting their daughter, for example. The veil of secrecy is lifted dramatically and the offender must now face the anxiety of possible rejection from those who are most important to him.
The client is instructed that he must assume responsibility for narrating and critiquing the film for his spouse. Just before viewing, the therapist should re-verify that the client is voluntarily asking his wife to watch the film.
As the film progresses, the therapist should subtly prod the client to comment. Simply stating, “What do you see there?” “Explain your excuses,” etc., sets the mood for the client to critically comment upon his performance. Wickramasekera (1980) found that causing the client to take a “critical analytic pedestrian” view of his deviancy helped him to understand and destroy distortions and fantasies which served as mediators for his abuse. The therapist should not rescue the client from the painful experience of fully explaining his deviance.
Stopping the film, rewinding, repeating a sequence over several times may be necessary before the client explains the sequence correctly.
Frequent questions can be expected from the outside observer; however, the visitor may be hesitant to stop the film and disrupt the sequence. The therapist should instruct the visitor-viewer to signal anytime there is a question. These interruptions serve to further force the client to discuss his behavior and take full responsibility. Allowing the film to roll nonstop can allow the client to avoid and “escape” the impact of public disclosure.
Client Selection
Wickramasekera (1980) cites four types of contraindications for his ABR procedure: psychotic, sociopathic, physically fragile to stress, and those unable to recognize and express fantasy material. These do not appear to pose severe limitations for the MABR procedure in a specialized outpatient setting. Psychotic sex offenders are not generally seen in such a setting, and similarly those unable to retrieve fantasy material are not generally treated in the usual program, either, although exclusion from MABR does not appear logical for this reason alone. Sociopathic personality disordered clients are generally resistant to most psychotherapy. MABR will not harm these clients, and it may be the only treatment that has impact. Those clients who have severe limitations, such as heart conditions, should be cleared and released through an M.D. prior to volunteering for the procedure.
MABR Timing
It appears most beneficial to institute MABR after the client has done considerable work to understand his pattern of offending, and reduce defensiveness. The ideal may not always be possible and MABR can be viewed as a “last resort” treatment for those clients who are not changing and appear at risk to re-offend.
When MABR is used with a resistant client or with the rare client very early in treatment, it is necessary to modify the sequence sessions and lengthen the procedure. The typical modification consists of shorter filming sessions followed by longer viewing phases. The viewing sessions will be used as examples for confrontation of the client’s treatment resistance. Two or three hours may be required before the Session 1 objectives are successfully accomplished and likewise for the remaining sessions. Extra care should be taken during the review of the film to ensure that the client attends to the film, learns and accepts. Frequent confrontation, questions, and demands on the client can help. GSR monitoring can also detect when a client is escaping from the impact of the technique. A simple portable unit can be used for this purpose.
Follow-Up
The videotapes become part of the client’s permanent file and should be used for regular follow-up contacts. Portions may be edited’to “set the tone” of the interview and thereby structure the follow-up session to the serious issues of the client’s attempts to control his deviancy. In some instances, merely running the entire film should be enough to provide an adequate “booster” to the client.
Outcome
Data presented in this section represents neither clean nor elegant empirical experimental design. The method of outcome data collection is open to criticism as is the obvious confounding of the design. The subjects involved here went through a complete and comprehensive program of treatment for their sexual behavior problem. At a minimum, all subjects were also involved in a long-term highly confrontive specialized sex offender group program as well as a number of other specific behavioral techniques. This includes covert sensitization, odor aversion, cognitive restructuring, and boredom aversion. Some clients also received extensive treatment for substance abuse problems, sexual dysfunction treatment, marital and family treatment, and communication, assertion skills, and hetterosocial skills training. Clearly a positive outcome could be readily attributed to these other procedures or to some, as of yet, unknown or unspecified factor.
Outcome data collection also suffers from considerable methodological problems. Whether or not the subject has re-offended is based upon either client self-report or our gaining this knowledge from some third party such as family member or police report. Not having access to confidential arrest records and files, we could not run a systematic records check on these individuals. However, in at least partial defense, we function within a very tight-knit and cooperative community. There is a high likelihood that if the individual were apprehended within the Puget Sound area we would be informed either by the police authorities, via inquiry from another therapeutic agency, by Children’s Protective Services or other types of network agencies. In a situation where the individual might leave the Puget Sound area after treatment, the probability of reporting of re-offense would be somewhat lowered. It should be noted that in four of the seven cases of re-offense, information came directly from the client himself or his family. Clients were typically seen for a period of eighteen months in continued treatment and treatment follow-up subsequent to their involvement in MABR. Clients “graduating” from the program are required to take a polygraph examination at the point of their successful termination, therefore data from at least this eighteen month period has some cross-checking and validity involved. There is in the outcome data also a small “control” group of individuals who refused participation in the MABR procedure.
This small group (n = 10) went through exactly the same procedures as the subjects accepting MABR with the exception of this one procedure. Use of this sample as a control group could be readily criticized based on the fact that these individuals were, in all probability, displaying a much lower motivational level. The present data is not offered to “prove” anything. Other researchers functioning in a situation much more conducive to an empirical experimental approach have already done the basic work with unconfounded subjects giving strong indication of the efficacy of the technique. The present data is intended simply to provide corroboration for the work of these other investigators.
A perusal of Table I indicates that 144 clients completed MABR. Of those, seven re-offended during the mean 24-month period after completion of the procedure. This is approximately five percent of the total number of individuals who elected to go through the procedure overall.
Table II indicates that of the ten individuals refusing participation in MABR, two re-offended within a sixteen month follow-up period after the date of their refusal. Twenty percent of these individuals are known to have re-offended.
Table II: Outcome of MABR “Refusers”
After a Mean Follow-Up of Sixteen Months
| Offense Behavior | Number | Reoffend | % Known Reoffenders | Mean # of Victims |
| Heterosexual child molester | 8 | 1 | 13.5 | 3.0 |
| Child rapist | 1 | 0 | 0 | 1.0 |
| Voyeurs | 1 | 1 | 100 | 10,000.0 |
| Exhibitionists | 3 | 1 | 33 | 366.0 |
| Total | 10{15} | 2{16} | 20 |
| Mean Follow Up | 16 Months |
| Range | 1–26 Months |
Discussion
In looking at those individuals who have re-offended, data specific to them is broken down in Table III.
As might be logically expected, high-frequency, low-risk behaviors such as exhibitionism encompass the bulk of the re-offense behavior. Motivation should be seen as a relevant variable. One hundred percent of the individuals re-offending in the acceptor sample had a negative termination status, either having unilaterally terminated the program against advice or having been terminated by the agency for lack of sufficient cooperation. Only 23% of the non-re-offenders have multiple primary paraphiliac diagnoses. Seventy-one percent of the failure sample had such multiple diagnoses while only 14% of the non-re-offenders were similarly classified.
Within some of the offender categories, in the minds of the authors at any rate, the results seem excessively exaggerated. The categories of male homosexual child molesters and bisexual child molesters have, within the literature, consistently yielded poor response to treatment and high probability of recidivism. In the present study, none of these individuals are known re-offenders. It is expected that, as these clients are followed over time, they will show significant rates of relapse.
Table III: Known Reoffenders
| Offense Behavior | Treatment Status | Re-offense | New Arrests | |
| S1 |
Breast Grabber Exhibitionist |
Terminated against advice | Expose | No |
| S2 |
Exhibitionist Predatory Female child molester |
Terminated against advice |
Expose Child Molestation |
Yes |
| S3 |
Exhibitionist Voyeur |
Terminated against advice Returned to treatment after rearrest | Expose | Yes |
| S4 | Child Rapist Child Molester | Terminated against advice | Attempted Child Rape | Yes |
| S5 | Exhibitionist | Terminated: Lack of Cooperation | Expose | No |
| S6 | Cross Dresser-Thief | Terminated against advice | Cross Dress/Steal | No |
| S7 | Exhibitionist/Obscene Phone Caller | Terminated: Lack of Cooperation | Expose/Obscene No Phone Call | No |
| % of Re-offenders Having Negative Termination Status | 100% |
| % of Non-re-offenders Having Negative Termination Status | 23% |
| % of Re-offenders Having Multiple Deviances | 71% |
| % of Non-re-offenders Having Multiple Deviances | 14% |
Maletsky (1980) makes the valid point that for a specific treatment procedure to be useful, it must have a fairly high rate of acceptance where offered to a specific client group. Citing his own experience as well as other studies published to that date, he makes the point that of thirty patients offered Aversive Behavioral Rehearsal, twenty-two refused it, yielding a refusal rate of 73%. In the present study of those one hundred fifty-four consecutive individuals offered the procedure, only ten declined, yielding a refusal rate of 7%. This is attributed to two factors. First, individuals are offered the program only after they have approximately six months of experience in an overall comprehensive program for the treatment of sexual deviance. They are used to dealing with their maladaptive behavior on a fairly direct basis and are usually past the stage where resistance and denial are major complications of the treatment process. The second major factor in the high acceptance rate noted may be the. fact that both the audience and the overt nudity factors have been eliminated. It is felt that this reduces the negative expectation level of the client, even though the replacements for these factors may be as emotionally impactful.
Wickramasekera (1980) reports approximately 17% of his cases experience severe negative side effects. These include anxiety reactions, suicidal ideation, clinical depression, recurrent nightmares, and impotence. To date, we have had no reports of such negative side effects within our sample. Clients will report feeling “down” for temporary periods, they will report anxiety while viewing themselves going through the procedure, they will report guilt, shame, self-disgust, self-anger, disinterest in sex, and embarrassment, but they do not report clinical symptomology. This may be, again, attributed to the fact that the procedure is used as a part of an overall treatment program and that the clients are quite experienced in terms of dealing directly with their behavior before the MABR procedure is ever instituted.
Summary
The above article has attempted to describe specifically a procedure adapted from Wickramasekera’s Aversive Behavioral Rehearsal modified for more economy and ease of presentation and utilized in a large community treatment program for sex offenders. The use of mannequins is advocated to enhance the reality and impact of the procedure and it is adapted for use with paraphilias other than exhibitionists. Data is presented on one hundred fifty-four cases wherein only 5% of those completing the procedure are known to have re-offended over a mean two year follow-up period.
A small control group of ten individuals refusing the procedure but going through all of the other components of the program showed a 20% rate of known re-offense over a lesser period of follow-up time. Modifications made to the procedure seem to reduce the incidence of negative side effects and enhance the level of both client and community acceptance of the procedure. Given the relative ease and economy of employing the procedure, it is felt that it can be readily incorporated into any sexual offender treatment program with the result of increasing the overall efficacy of the total approach.
References
Cox, D. J. & Daitzman, R. J. (Eds.). (1980). Exhibitionism: Description, assessment and treatment. New York: Appleton-Croft.
Forgione, A. G. (1976). The use of mannequins in the behavioral assessment of child molesters: Two case reports. Behavior Therapy, 7, 678–685.
Jones, I. V. & Frei, D. (1977). Provoked anxiety as a treatment of exhibitionism. British Journal of Psychiatry, 131, 295–300.
Maletsky, B. M. (1980). Assisted covert sensitization. In Cox, D. J. & Daitzman, R. J. (Eds.). Exhibitionism: Description, assessment and treatment. New York: Appleton-Croft.
Reitz, W. E. & Keil, W. B. (1971). Behavioral treatment of an exhibitionist. Journal of Behavioral Therapy and Experimental Psychiatry, 2, 67–69.
Serber, M. (1970). Shame aversion therapy. Behavioral Therapy and Experimental Psychiatry, 1, 167–176.
Stevenson, J. & Jones, I. H. (1972). Behavior therapy techniques for exhibitionism. Archives of General Psychiatry, 27, 239–241.
Wickramasekera, I. (1976). Aversive behavioral rehearsal for sexual exhibitionism. Behavior Therapy, 7, 167–176.
Wickramasekera, I. (1980). Aversive behavioral rehearsal: A cognitive behavioral procedure. In Cox, D. J. & Daitzman, R. J. (Eds.). Exhibitionism: Description, assessment and treatment. New York: Appleton-Croft.
Afterword
Dennis M. Dailey
After my own reading of the manuscripts contained in this volume, I was struck by several matters in ways never quite like before.
I have known throughout my career as a social worker and sexologist that professional life is frequently burdened by major gaps in knowledge and intervention strategies. In so many ways we do not know all that much about the sexual dimension of the human condition. Knowledge and intervention gaps seem especially apparent as it relates to the sexually unusual. There are still so many research questions remaining to be addressed, and serious help for the sexually unusual is relatively recent. That is, help that is really helpful. The paradox is that we do know some things, but not all of us in the helping professions have an equal grasp of what exists and what constitutes realistic intervention options.
If today’s helping professionals could refine their practice by not treating all of the sexually unusual as if they were the same, some gain will have been made. Just restraint in using “sick/weird” or criminal labels inappropriately would free the genuine helper to bring more richness to the helping encounter. Just recognizing that those persons who are in the sexually unusual group, who either need or desire help, can in fact be helped will reduce the hopelessness that seems so often attached to their struggle for fullness of life.
The helping professionals who can begin to incorporate into their awareness the enormous variety that occurs in sexual expression will interact differently with the fetishist or sadomasochist who simply needs affirmation, information, and options. Likewise, persons whose expression of sexual variability is coercive and nonmutual or uncomfortable to themselves will encounter the professional helper who has more compassion, and the clients will experience less judgmentalism and punitive interactions. Too often those who experience the need or desire for help in sex-related concerns encounter helpers who reflect the harsh, judgmental, inaccurate, and narrow perspectives on sexuality which still exist in our society, despite what some feel regarding the impact of the so-called sexual revolution. Too often the sexually unusual do not experience helpful encounters, but in fact are frequently harmed by the “helping” process.
Let me close this search with a quote from one of the more useful texts for the helping professional, entitled The Velveteen Rabbit (1982):
... once you are Real you can’t be ugly, except to people who don’t understand.
The sexually unusual are Real. As we see their realness, we cease to see them only as ugly. Those who understand will be helpful. Those who do not understand cannot be helpful. And above all — FIRST DO NO HARM.
Reference
Williams, M. (1982). The Velveteen Rabbit. Philadelphia: Running Press.
Subject Index
A
Acrotomophilia, 16 Addiction Carnes model, 98 sexual, 7–10,131–147 Adolescence
development of sexual aggression, 133 and Obscene Phone Callers, 126 and non-deviant arousal, 97 Aggression
and Obscene Phone Callers, 122 sexual, 131–147 and S/M, 44 Alcoholism
in Exhibitionism/Voyeurism, 101 in Pedophilia, 91,92,99 in Transvestism, 60–62 Anorgasmia, 6,9 Arousal
and Fetishism, 27–28,36–37 and Obscene Phone Callers, 113 and Pedophilia, 91–97,99–100, and S/M, 53 and Transsexualism, 79 and Transvestism, 58,59–62,67 Assertiveness
skills for Pcdophiliacs, 94–95,98 Auonicpamperphilia, 16 Auoniepipphiliac, 16 Aversion
conditioning, 94–96,149 to genital touch, 79
B
Bestiality, 16,22 Bisexuality defined, 60
in S/M, 46
in Transsexualism, 79 in Transvestism, 61 Bondage, 48,55 Buggery, 16,22
C
Compulsivity, 70,132,151 Coprophilia, 113 Cross-dressing, 57–73 Cross-gender, 62,78 Cross-living, 85 Cross-sex, 60 Cunnilingus, 22
D
Depression
in sexual aggression, 131–135 in S/M, 20
in Transsexualism, 79–80,83
E
Egodystonic homosexuality, 51,79–80 Electrolysis, 61 Enema, 113 Eonism, 16,58 Epilepsy, 127,129 Exhibitionism, 8–9,63,101–111,114, 117–119,128,149–155 definition, 102 etiology, 102–104 in history, 11–13
patterns and characteristics, 104–109 treatment of, 109–111
F
Fantasy
and aggression, 129,136–141,142–145 and behavior, 110 diary, 98
in Fetishism, 28–29,32,37 masturbatory, 134–135 in Obscene Phone Callers, 118–122 in Pedophilia, 91–92,95–97 in S/M, 47
in Transvestism, 61,68 Fetishism, 27–42
and Obscene Phone Callers, 118,127 and S/M, 46
and Transvestism, 57,76,78–79 Frottage, 116
G
Gender Dysphoria, 77–80,83–86 Gender Identity defined, 59 Gender Role defined, 59–60
H
Hermaphroditism, 23–24,73–74 History, 15–24 and religion, 15,17 of S/M, 45–46 of Transvestism, 57–58 Homophobia, 11,68 Homosexuality defined, 60 in DSM III, 22–23 in history, 15–16 in Pedophilia, 99 in S/M, 45–46,51 in Transvestism, 58–60,61,68 in Transsexualism, 77–79 Hypersexuality, 127,129 Hyper-masculinity, 20
I
Impotence, 117,123,163
Incest, 91–92,98,101,135,144,147–148
Inhibition and sexual aggression, 132–133, 135–138,143–144,148
K
Klismaphilia, 113 L
Leathersex, 20,24 Lesbianism in S/M, 46
in Transvestism, 66–68
M
Masochist, 44–45
MMPI, 84,103,106–107,112,134,146 Modeling, 98
Modified Aversive Behavioral Rehearsal (MABR), 151–164 Mysophilia, 113
N
Necrophilia, 113 O
Obscene Phone Callers behavior patterns, 113–114 definition, 113–115 and Exhibitionism, 115 and fantasy, 119–120 treatment of, 123–126 and women victims, 122–123 Olfactorophilia, 17 Overt aversive techniques, 96–97 Overt sensitization, 163
P
Paraphilia, 9–11,16–18,27–28,91–92,113, 149–150,163 Pedophilia, defined, 92 and incest, 93
and Obscene Phone Callers, 114,118 treatment of, 94–100,151–154 Peniligus, 22
Penile Plethysmography, 103,142,146 Polygraph, 96,146,160
R
Reparenting, 146–147 Reproductive Bias, 6–8
Sadomasochism, 8–9,10–13,43–55 behaviors, 48–50 clinical problems, 50–54 defined, 44–45 etiology, 44–45 history of, 45–46 practitioners of, 46–48
Scatalogia, 113–114
Sodomy, 15–16
Sexual abuse and MABR, 154–155,156,158 in Pedophilia, 95 in S/M, 53–54 in Transsexualism, 79 in Transvestism, 63 aggression and addiction, 131–147 treatment of, 149–164 addiction and aggression, 131–147 as a diagnotic category, 8–10 oppression, 6–10 defined, 6–7 reassignment surgery, 77–87 unusual, 6–10, 11–12**
Transgender, 57, 62, 63–64, 70, 73–74, 84–85, 86
Transsexualism, 8–9,77–87 defined, 77–79 and egodystonic homosexuality, 78–79 in history, 17,18 standards of care for, 80–83 treatment of, 83–86 Transvestism, 8,11–12,56–73 defined, 60–61 and Fetishism, 36,38 in history, 16–20 treating couples, 71–72 treatment of, 62–66 women partners of men with, 66–71
Uranism, 58 Urophilia, 113
Vaginismus, 6,10
Voyeurism, 8–9, 11, 28, 101–112, 118, 162–164 defined, 102 etiology, 102–104 patterns and characteristics of, 104–109 treatment of, 109–111
[1] Other terms include D/S (Dominance and Submission), B/D (Bondage and Discipline), kinky sex, corporal punishment, top and bottom play, M/S (Master and Slave), leathersex, etc.
[2] There are some incidences of problems occurring from clearly accidental circumstances. For example, someone contracted an infection after having her nipple pierced. Efforts were made to do piercing under sterile conditions by appropriately trained personnel; nevertheless an infection occurred. Since the infection was not intentional nor due to negligence, it is classified as accidental. It should be noted that most sports (and sexual) activities have accidental injuries associated with their practice.
[3] The hot wax used by S/M practitioners is usually paraffin which does not bum. The more expensive beeswax candles can burn and for that reason are rarely used.
[4] It seems likely that any injuries clearly related to an S/M interaction would be reported by the press. Similar events (e.g., reports of light bulbs found in a patient’s rectum or kidnaping of a woman as a “sex slave”) have received more coverage than would be expected by the seriousness of the problem. The lack of stories in the press concerning S/M related injuries and the lack of its mention in other professional journals suggest that the actual occurrence is rare.
[5] Throughout this chapter, the term transgender will be used to refer to the broad category of behavior where persons of one sex emulate or take on attributes of the other sex. In this context, transvestism and transsexualism are forms of transgender behavior.
[6] Such anomalies are beyond the scope of this section. For more details, refer to texts such as Money (1968) and Green and Money (1969).
[7] The latter might occur when a transsexual male was instructed to cross-dress as a part of his gender reassignment regimen.
[8] For more complete information on the development of these categories the reader is referred to Kinsey et al. (1948).
[9] Specifically excluded from these definitions are those situations that are caused by genetic, anatomical or hormonal causes such as hermaphroditism.
[10] The approaches suggested below are not generally applicable for treatment of transsexual persons although they will not cause harm. In some cases a client may present himself as a cross-dresser and later it may become “obvious” that he is more probably transsexual. In such cases, the clinician is advised to make contact with a gender clinic for specialized help. For such guidance contact J2CP Information Services, P.O. Box 184, San Juan Capistrano, CA 92693–0184, who can provide referrals for most of the country.
[11] The masculine pronoun will be used here because the phenomenon being discussed is male-oriented. There is no implied or overt sexism in this terminology-
[12] The details of taking such a history are beyond the scope of this chapter. The reader is referred to Taking a Sex History by Pomeroy, Flax, and Wheeler for a good treatise on this subject.
[13] Any medical problem uncovered during the history taking must be treated or referred for treatment. Any medications being taken should be checked for potential influences on sexual functioning or behavior. A Comprehensive guide for the effects of drugs on sexual functioning is Drug, Alcohol and Sex by Bush.
[14] The treatment for a transsexual client will not be covered in this chapter. The Harry Benjamin International Gender Dysphoria Association has established Standards of Care for such situations. These can be found in Archives of Sexual Behavior 14: 79–90, Februaiy 1985.
[15] In some cases, the woman will refuse to present herself for counseling and may not even be aware of her husband’s cross-dressing. In the latter case, whether or not she should be told may be one of the issues that is worked on during therapy. There are many apparently successful marriages where the women never knows of her husband’s penchant for wearing women’s clothing.
[16] While this discussion is beyond the scope of this chapter, the reader is referred to texts such as Sexual Interactions by Allgeier and Allgeier for a comprehensive examination of role development.
[17] The following technique equally well applies if the man decides, during the course of therapy, to tell the woman he is in a relationship.
[18] The best reference for locating such groups is TV-TS Tapestry, P. O. Box 19, Wayland, Massachusetts 01778. This magazine also has many good articles dealing with all manner of transgender issues.
[19] It is probably not appropriate to have the man cross-dressed for any of the joint sessions. If it seems necessary, the same rules should be followed as previously stated: he should cross-dress after arrival and not leave cross-dressed.
{1} Address reprint requests to Dr. Dennis M. Dailey, School of Social Welfare, Twente Hall, The University of Kansas, Lawrence, Kansas 66045.
{2} Address reprint requests to Dr. Vern L. Bullough, Dean, Faculty of Natural and Social Sciences, State University College at Buffalo, 1300 Elmwood Avenue, Buffalo, NY 14222. © 1988 by The Haworth Press, Inc. All rights reserved.
{3} Address reprint requests to Thomas 0. Sargent, Designed Change Institute, 3 Columbia Street, Hartford, CT 06106.
{4} Address reprint requests to Dr. Charles Moser, 2200 Benjamin Franklin Parkway, # E1702, Philadelphia, PA 19130.
© 1988 by The Haworth Press, Inc. All rights reserved.
{5} Address reprint requests to Dr. Roger E. Peo, P.O. Box 4887, Poughkeepsie, NY 12602.
© 1988 by The Haworth Press, Inc. All rights reserved.
{6} Address reprint requests to Dr. Sharon B. Satterfield, Program in Human Sexuality, University of Minnesota, Research East Building, 2630 University Avenue, SE, Minneapolis, MN 55414.
© 1988 by The Haworth Press, Inc. All rights reserved.
{7} © 1988 by The Haworth Press, Inc. All rights reserved.
{8} Address reprint requests to Dr. Edward L. Rowan, 6 D Hill Avenue, Concord, NH 03301.
© 1988 by The Haworth Press, Inc. All rights reserved.
{9} Address reprint requests to Margretta Dwyer, Program in Human Sexuality, University of Minnesota, Research East Building, 2630 University Avenue, SE, Minneapolis, MN 55414.
© 1988 by The Haworth Press, Inc. All rights reserved.
{10} K scale & is based on a score lower than 40 t score.
{11} Address reprint requests to Ord Matek, Associate Professor Emeritus, Jane Addams Graduate School of Social Work, University of Illinois —Chicago, Chicago Circle, P.O. Box 4348, Chicago, IL 60680.
© 1988 by The Haworth Press, Inc. All rights reserved.
{12} Address reprint requests to Steven C. Wolf, Northwest Treatment Associates, 315 West Galer Street, Seattle, WA 98119.
© 1988 by The Haworth Press, Inc. All rights reserved.
{13} Address reprint requests to Timothy A. Smith and Roger W. Wolfe at Northwest Treatment Associates, 315 West Galer Street, Seattle, WA 98119.
© 1988 by The Haworth Press, Inc. All rights reserved.
{14} Many sexual offenders have multiple deviances and are listed more than once.
{15} Many sexual offenders have multiple deviances and are listed more than once.
{16} Ibid.