Luigi Mangione’s handwritten notes on his back pain & injury
2019-05-18
From Luigi to Jules — On living with chronic back pain — 2025
Sources:
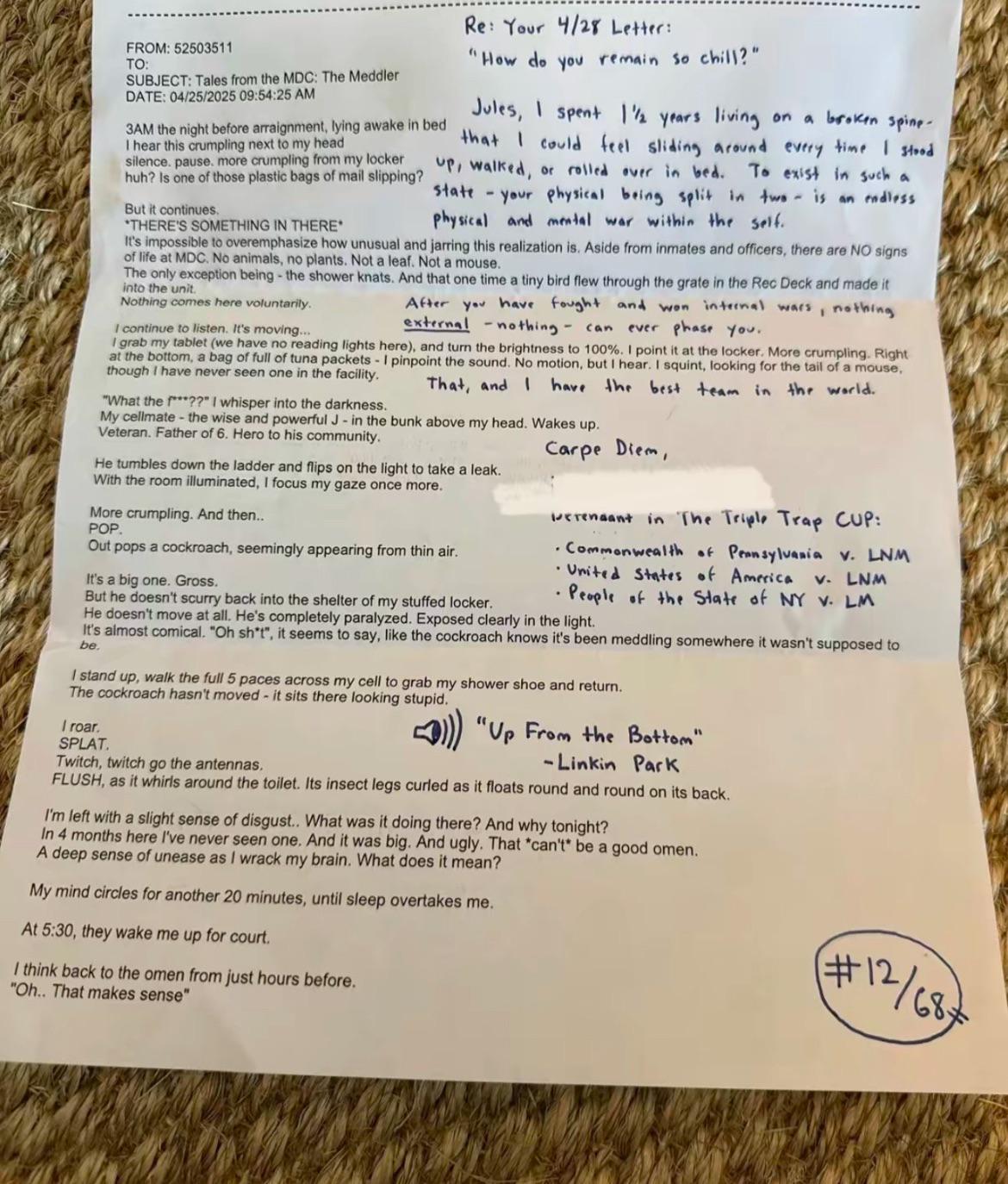
Re: Your 4/28 Letter:
“How do you remain so chill?”
Jules, I spent 1 ½ years living on a broken spine that I could feel sliding around every time I stood up, walked, or rolled over in bed. To exist in such a state — your physical being split in two — is an endless physical and mental war within the self.
After you have fought and won internal wars, nothing external — nothing — can ever phase you.
That, and I have the best team in the world.
Carpe Diem,
Luigi Mangione
Review of ‘Bigger Leaner Stronger’ — May 18, 2019
Source: <defenderofbasic.github.io/luigi-mangione-storyline/books/goodreads-read.html>
Title: Bigger Leaner Stronger: The Simple Science of Building the Ultimate Male Body
Author: Michael Matthews
Read: 2019-09-??
Added: 2019-05-18
Rated: ★★★★
The introduction to weightlifting.
Fantastic, clear content.
-1 star: too infomercial, too aesthetics-focused
My written notes: https://drive.google.com/file/d/1Fxje...
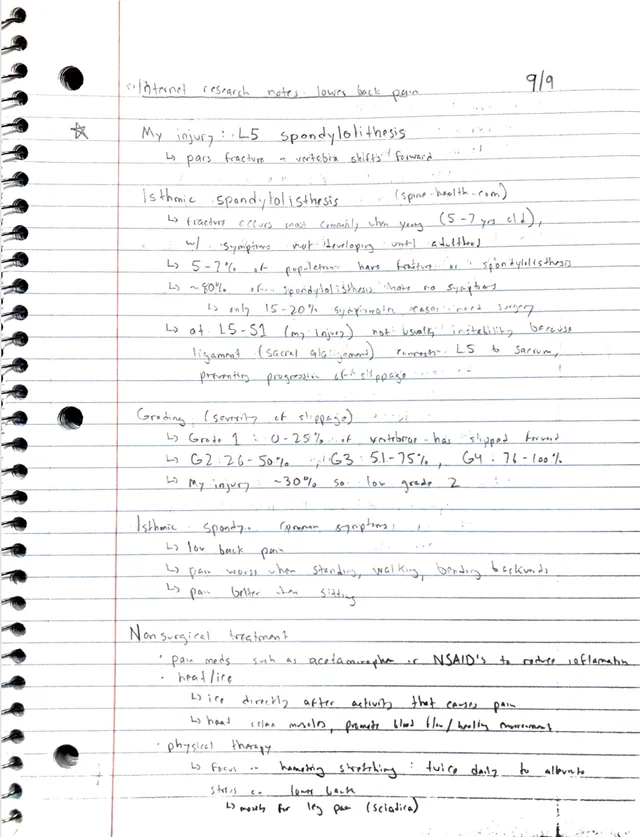
Internal research notes – Lower back pain
My injury: L5 Spondylolisthesis
-
Pars fracture → vertebra slippage/fracture
Isthmic Spondylolisthesis (spon-do-lis-the-sis)
-
Repetitive stress most commonly when young (5–7 years old),
-
symptoms not developing until adulthood
-
-
5–7% of the population has pars fractures or spondylolisthesis
-
80% of those with spondylolysis have progression to slippage
-
is only 15–20% become symptomatic enough to require surgery
-
-
of L5-S1 (my injury) not usual instability because ligamental (sacral alignment) prevents L5 from slipping further onto sacrum.
Grading (Severity of slippage):
-
Grade 1: 0–25% of vertebra has slipped forward
-
Grade 2: 26–50%
-
Grade 3: 51–75%
-
Grade 4: 76–100%
-
My injury: ~30% slip → Low Grade 2 Common symptoms of Isthmic Spondylolisthesis:
-
Low back pain
-
Pain worsens with:
-
Standing
-
Walking
-
Bending backward
-
Pain improves with: Sitting Non-Surgical Treatment:
-
Pain medications:
-
Acetaminophen or NSAIDs to reduce inflammation
-
Heat/ice therapy:
-
Ice directly after activities that cause pain
-
Heat before motion to promote blood flow/muscle relaxation
-
Physical Therapy:
-
Focus on muscle strengthening and stretching (twice daily)
-
Stretching lower back
-
Mostly for leg pain (sciatica)
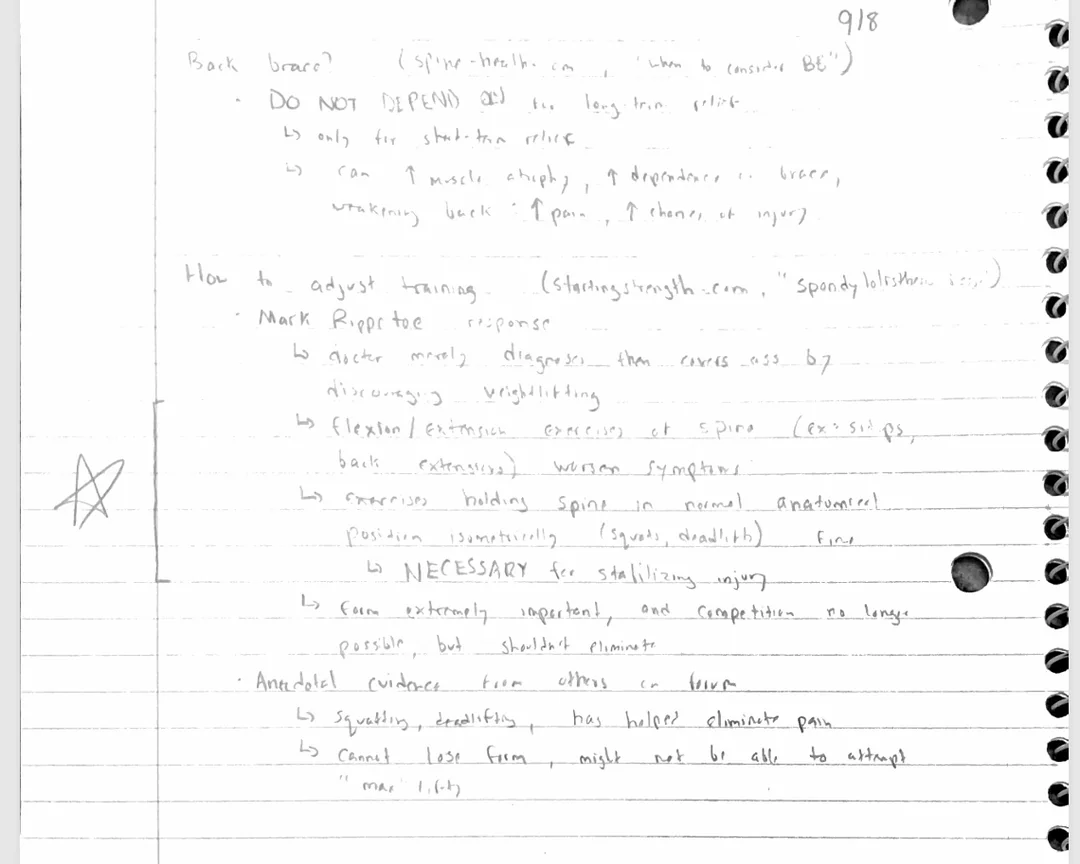
Back Brace?
-
DO NOT DEPEND ON IT
-
Only for short-term relief
-
Long-term use can weaken muscles, leading to:
-
Increased muscle atrophy
-
Increased dependence on brace
-
Increased pain & chance of injury
How to adjust training?
(Source: StartingStrength.com – “Spondylolisthesis & Lifting”)
-
Mark Rippetoe’s response:
-
Acute models diagnose this then correct it by discouraging weightlifting
-
Extension exercises worsen symptoms (e.g., sit-ups, back extensions)
-
Corrective approach:
-
Hold the spine in a neutral anatomical position (isometric stabilization, e.g., squats, deadlifts)
-
NECESSARY for stabilizing injury
-
Competing at high intensity → No longer possible, but weightlifting should not be completely eliminated
-
Anecdotal evidence from others with spondylolisthesis:
-
Squatting, deadlifting helped eliminate pain
-
Caveat:
-
Cannot lose form – might not be able to attempt max lifts
Summary of Key Points:
-
L5 Spondylolisthesis (Low Grade 2, ~30% slip)
-
Symptoms: Low back pain, worse with standing/walking, better with sitting.
-
Non-surgical treatments: NSAIDs, ice/heat, PT (stretching & strengthening).
-
Bracing: Only for short-term; long-term use weakens muscles.
-
Training: Avoid hyperextension, focus on neutral spine stability (e.g., squats, deadlifts).